Choosing the wrong behavioral health EMR can lead to inefficiencies, clinician burnout, legal risks, and poor patient outcomes.
Here's what to watch out for:
Limited customization: Systems designed for primary care often don't fit behavioral health workflows, forcing workarounds that waste time.
Poor integration: Lack of connectivity with labs, telehealth, or e-prescribing tools creates data silos and disrupts care.
Weak compliance and security: Missing features for regulations like 42 CFR Part 2 or HIPAA can result in hefty fines and legal issues.
No clinical decision support: Without tools like automated assessments or outcome tracking, care quality suffers.
Scalability issues: Systems that can't handle growth or remote access limit your practice's potential.Avoid these pitfalls by prioritizing behavioral health-specific features, compliance tools, seamless integrations, and scalability when evaluating EMR vendors.
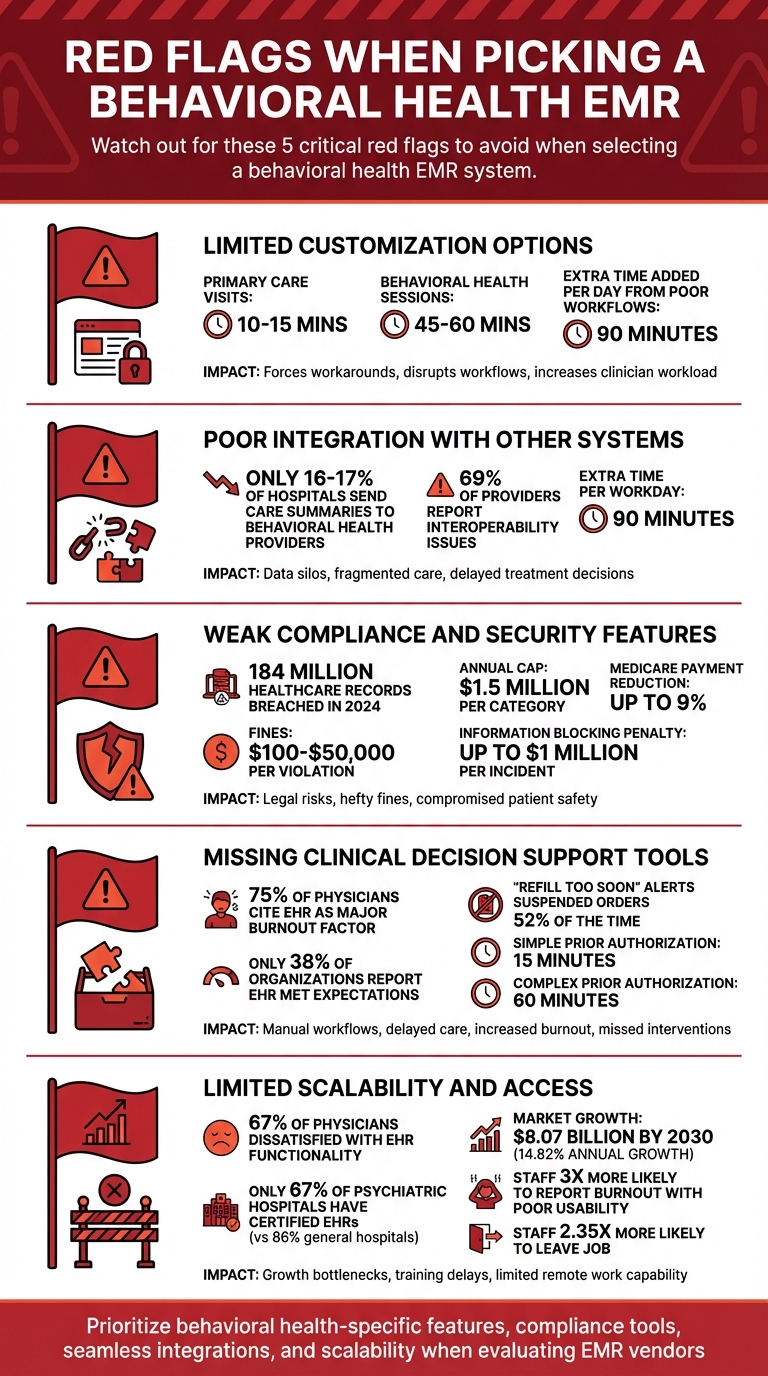
5 Critical Red Flags When Choosing Behavioral Health EMR Systems
Strategically Address Behavioral Health EHR Challenges | Select, Optimize, Implement Your EHR
Red Flag 1: Limited Customization Options
When an EHR system offers limited customization, it forces clinicians to adapt to generic workflows tailored for quick 10–15 minute primary care visits.
This approach clashes with the 45–60 minute sessions common in behavioral health care, leaving providers stuck with inefficient processes instead of receiving meaningful support for their work[5].
The problem becomes even more pronounced when the system lacks specific fields for essential tasks like ASAM criteria, Medication-Assisted Treatment (MAT) tracking, and group therapy documentation.
Without these tools, tracking attendance and outcomes turns into a logistical headache[1][3].
Clinicians often resort to creating workarounds or inputting critical information into generic text fields that fail to capture the depth and nuance required in behavioral health care. This rigidity disrupts daily workflows, making it harder for providers to focus on patient care.
How It Affects Clinical Workflows:
"When practices choose a 'popular' EHR without confirming it has behavioral health templates and assessment tools, documentation becomes a daily struggle. The system fights against your workflow instead of supporting it."
– PIMSY Team[5]
Non-customizable systems lead to inefficiencies that quickly add up. For instance, during vendor demonstrations, observe how many clicks it takes to perform routine tasks like starting a telehealth session or completing a progress note[5].
Each additional click increases clinician workload. In group therapy settings, the inability to document multiple clients in a single note forces providers into repetitive data entry, wasting valuable time[3].
To improve efficiency, it's worth seeking systems that integrate tools like PHQ-9 and GAD-7 directly into the workflow. When these tools are separate questionnaires requiring manual entry, they add another layer of inefficiency that disrupts the system’s ability to support unique care models[5].
Lost Opportunities for Personalization:
Rigid EHR systems also limit the ability to align the software with your organization’s specific treatment approaches.
For example, behavioral health practices often rely on frameworks like the Problem-Goal-Objective-Intervention (PGOI) structure or need adjustable review intervals for substance use disorder treatment. Without configurable fields to support these models, the system fails to meet the demands of behavioral health care[3].
Additionally, the lack of customization hinders outcome tracking. Systems that cannot adapt to evolving treatment plans or configure ASAM multi-dimensional assessments leave clinicians stuck with static data.
Behavioral health care requires dynamic tools to monitor patient progress over time, and without these, continuity of care and accurate progress tracking suffer[3]. Customization isn’t just a convenience - it’s a necessity for operational efficiency and delivering high-quality care.
Red Flag 2: Poor Integration with Other Systems
When an EMR struggles to integrate with other systems - like labs, telehealth platforms, or e-prescribing tools - it creates data silos that disrupt patient care and drain clinician efficiency. This isn't just inconvenient; it's risky.
A lack of interoperability can lead to fragmented information, putting patients at greater risk. With federal regulations like USCDI v3 and the 42 CFR Part 2 single-consent requirements (effective February 16, 2026), interoperability is now a mandatory standard, not just a nice-to-have feature[12].
Yet, the numbers tell a troubling story: only 16–17% of hospitals regularly send care summaries to behavioral health providers, the lowest rate across all care settings[12].
One major issue is when prescribers can't access a patient's complete medication history. Without integration between EMR and e-prescribing systems, clinicians are forced to make decisions based on partial data, increasing the potential for harmful drug interactions[12].
Similarly, if lab results arrive via fax instead of flowing directly into the patient's record, delays in clinical decision-making and treatment adjustments become inevitable[12]. This lack of integration doesn't just slow things down - it puts patient safety at risk and disrupts the clinical workflow.
Data Silos and Disconnected Care:
"A prescriber who can't see a patient's full medication history is making decisions with incomplete information. That's a patient safety problem."
– The PIMSY Team[12]
Disconnected systems create internal data silos that make coordinated care nearly impossible. For example, if a therapist uses one system for documentation and a psychiatrist uses another for prescriptions, the care team loses access to a shared clinical record[12].
Patients end up repeating their history to multiple providers or filling out the same demographic forms because intake portals don't sync with billing or clinical systems[12]. This inefficiency has a direct impact on clinicians, who spend over one-third of their week on documentation instead of patient care[13].
And it’s not just an isolated issue - 69% of healthcare providers report struggling with interoperability problems between their EHR and other systems[14].
Inefficiencies Across Multiple Systems:
When systems like calendars and clinical notes don’t sync, staff are left manually entering details - like session dates, times, and durations - into progress notes. This not only increases the chance of errors but also results in missed documentation and gaps in reporting[11].
To compensate, teams often rely on outdated workarounds like faxing, scanning, and phone calls to track down missing records, which eats into time that could be spent on patient care[13].
On top of that, poor integration with billing systems delays claims processing and disrupts cash flow[12]. These inefficiencies add up fast - misaligned EHR workflows can extend a provider’s workday by an average of 90 minutes[6].
|
Integration Type |
Risk of Poor Integration |
Impact on Care |
|---|---|---|
|
Labs |
Manual result entry |
Fragmented records; slower treatment adjustments |
|
Telehealth |
Managing separate platforms and manually transferring notes |
Reduced patient engagement; added administrative workload |
|
E-Prescribing |
Limited visibility into medication history |
Higher risk of contraindications and errors |
|
Billing/RCM |
Manual claim submissions |
Delayed revenue and cash flow issues |
|
Scheduling |
Disconnected calendar and documentation |
Missed notes; duplicate data entry; reporting gaps |
Red Flag 3: Weak Compliance and Security Features
When an EMR system lacks strong compliance and security measures, the risks extend far beyond operational hiccups. These gaps can lead to legal trouble, financial penalties, and compromised patient safety.
The numbers are alarming: in 2024, around 184 million healthcare records were breached[15]. For practices, this could mean fines ranging from $100 to $50,000 per violation, with annual caps hitting $1.5 million per category - even if the data breach happens on your own server[17]. Below, we’ll explore how weak compliance and security measures can jeopardize your practice.
Compliance Problems:
Falling short on compliance can result in costly penalties. For instance, psychiatrists billing $300,000 annually to Medicare could face a $27,000 adjustment (9%) if they fail to meet Promoting Interoperability standards like certified e-prescribing[8].
The stakes are even higher under the 21st Century Cures Act, where information blocking violations can cost up to $1 million per incident[8]. If your EMR lacks ONC certification (CEHRT), your practice might not meet the requirements for MIPS Promoting Interoperability or CCBHC certification[8].
Behavioral health practices have even stricter regulations. For example, 42 CFR Part 2 governs substance use disorder (SUD) records and requires granular consent management. It also mandates separating psychotherapy notes from other medical records, as per the Cures Act[8][15][16].
Without an EMR that can handle these workflows, practices risk criminal penalties and losing their SUD program licenses[15][16]. Additionally, the upcoming HTI-1 Final Rule (effective January 2026) will require certified EHRs to support USCDI v3, which includes sensitive data like social determinants of health and gender identity[8].
Data Security Issues:
Beyond compliance, weak security features can put sensitive patient data at risk.
An EMR without end-to-end encryption, multi-factor authentication (MFA), and comprehensive audit trails fails to meet the HIPAA Security Rule’s requirements for safeguarding electronic protected health information (ePHI)[1][16].
Audit logs, in particular, must automatically record every access, edit, or export to meet OCR audit standards[15].
For practices dealing with controlled substances, missing features like electronic prescribing of controlled substances (EPCS) with two-factor authentication and Prescription Drug Monitoring Program (PDMP) integration can pose significant risks to patient safety[8][17].
Many states now require prescribers to check PDMPs to prevent overdoses and "doctor shopping"[17]. If your EMR forces clinicians to leave the platform to access these databases, it disrupts workflows and increases the risk of dangerous prescribing errors.
Additionally, role-based access controls (RBAC) that ensure unique logins for every user are essential for meeting HIPAA’s unique user identification standards.
|
Standard/Regulation |
Focus Area |
Penalty/Risk of Non-Compliance |
|---|---|---|
|
HIPAA Security Rule |
Safeguards for ePHI (technical/physical) |
|
|
42 CFR Part 2 |
Consent and disclosure for SUD records |
|
|
Cures Act |
Information blocking and patient data access |
Up to $1 million per violation[8] |
|
MIPS (PI Category) |
Certified EHR technology use |
Up to 9% Medicare payment reduction[8] |
|
CCBHC Criteria |
Interoperability and quality reporting |
Loss of funding or status[8] |
Red Flag 4: Missing Clinical Decision Support and Outcomes Tools
When an EMR lacks clinical decision support (CDS) and outcomes tracking, it forces clinicians into time-consuming manual workflows. This not only delays care but also increases the chance of missing critical interventions.
Features like risk stratification, customizable alerts, and built-in assessments are essential for tracking patient progress and practicing measurement-based care effectively [4].
The absence of these tools adds to the documentation burden, which already weighs heavily on providers. Misaligned EHR workflows, often due to missing clinical tools, extend workdays and contribute to burnout.
In fact, 75% of physicians reporting burnout cite their EHR as a significant factor [6]. Without automated scoring for assessments like PHQ-9 or GAD-7, clinicians spend extra time calculating scores and retrieving forms - time that could be better spent with patients [5][6]. This inefficiency impacts not only day-to-day operations but also the overall quality of care.
Problems with Evidence-Based Practice:
A lack of CDS tools in an EMR creates serious gaps in care delivery. For example, systems without risk stratification can't automatically flag high-risk patients who may need urgent intervention for issues like relapse or self-harm [4].
Similarly, without customizable alerts, clinicians are left manually tracking key deadlines like compliance checks, authorization expirations, and medication coverage - leading to delays in care [18].
Real-time prescribing support is another critical feature. In 2021, "Refill too soon" alerts in an EHR prompted providers to suspend orders 52% of the time, helping avoid pharmacy issues and reducing inappropriate prescriptions [18].
Without such alerts, administrative tasks pile up. For example, processing a simple medication prior authorization takes about 15 minutes, while a complex one can take up to an hour when no integrated support tools are available [18].
"When providers have the right information at the point of care, they can provide a better experience by ensuring patients don't waste time at the pharmacy." – Arrive Health [18]
Regulatory changes are also raising the bar. Organizations like the Joint Commission now require Measurement-Based Care (MBC) models, which depend on standardized assessment tools to track outcomes [4].
Payers increasingly demand data to justify costs, leaving practices without these tools struggling to meet value-based care requirements [4]. For instance, CPT code 96127 allows brief behavioral assessments to generate 5% to 20% more revenue, but only if the EMR can systematically deliver and track these assessments [2].
No Way to Track Patient Outcomes:
Another major issue is the inability to track patient outcomes over time.
Behavioral health often requires monitoring progress over months or even years, but EMRs without longitudinal tracking tools make it nearly impossible to visualize whether a patient is improving or regressing [5]. Without integrated outcome measures, providers risk continuing ineffective treatments, ultimately compromising patient care [4][2].
"Measurement-Based Care is rapidly becoming the standard as payers request more data and better patient outcomes to bring down costs in behavioral and physical health." – Andrew Schatzberg, Valant [2]
The lack of integrated assessments also disrupts workflows. When tools like PHQ-9, GAD-7, and DAST-10 aren't embedded in the EMR, clinicians are forced to rely on paper forms or export data to Excel - interrupting care delivery and increasing the likelihood of data entry errors [5][6]. This fragmentation makes it difficult for practices to generate the quality reports required by CMS and other payers [5][1].
Here's a closer look at the missing features and their clinical impacts:
|
Feature |
Impact of Absence |
Clinical Risk |
|---|---|---|
|
Risk Stratification |
No automated flagging of high-risk patients |
Delayed intervention for relapse or self-harm [4] |
|
Customizable Alerts |
Manual tracking of compliance and care gaps |
Missed regulatory deadlines or authorization expirations [1][3] |
|
Outcome Tracking |
Inability to visualize patient progress |
|
|
Auto-Scoring Tools |
Manual calculation of PHQ-9/GAD-7 |
Increased administrative burnout and data entry errors [6] |
These missing capabilities prevent practices from meeting evolving standards of care. Only 38% of healthcare organizations report that their EHR implementation met initial expectations [9], often due to the absence of behavioral health tools.
Advanced EMRs now include features like relapse monitoring, which automatically flags high-risk patients based on assessment scores, enabling timely interventions [4]. Unfortunately, generic medical EMRs often fall short in providing these critical functionalities.
Red Flag 5: Limited Scalability and Access
Beyond compliance and clinical decision support challenges, issues with scalability and access can severely limit an EMR's ability to meet the demands of behavioral health care.
If your EMR can't grow with your organization or support remote work, it risks becoming a bottleneck for operations.
In fact, 67% of physicians report dissatisfaction with their EHR system's functionality [14], with scalability problems being a major contributing factor. A system that works for a small practice of five clinicians often becomes unmanageable when scaled to 50 or more providers, creating inefficiencies that slow everything down.
The behavioral health EHR market is expected to grow to $8.07 billion by 2030, with a 14.82% annual growth rate [20].
However, only 67% of psychiatric hospitals have adopted certified EHRs, compared to 86% of general acute care hospitals [20]. This disparity highlights how many systems fail to meet the demands of multi-location behavioral health operations.
Restrictions on Growth:
An EMR that lacks flexibility can make growth feel impossible.
Whether you're acquiring a new practice or opening a second location, you need a system that can seamlessly integrate patient data, billing workflows, and clinical records. Systems without multi-location support often require months of manual data integration, driving up operational costs as you expand [14].
"If you're avoiding growth opportunities because your technology can't support them, that's a clear sign you need a better platform." – ProsperityEHR [14]
Take the case of Beacon Outpatient Management in February 2026. With operations spanning eight states, they faced documentation bottlenecks that hindered their scalability.
Under the guidance of Tabatha Golding, Senior Vice President of Operations, they adopted AI-powered clinical documentation. This change reduced the average time spent on notes from 10–12 minutes to under 3 minutes, freeing staff to focus on patient care while maintaining documentation standards across states [20].
The financial strain of poor scalability isn't limited to lost growth opportunities. In growing practices, every new hire faces longer training periods when the system is unintuitive or inconsistent, further driving up costs [19].
Additionally, staff using systems with poor usability are 3 times more likely to report burnout and 2.35 times more likely to consider leaving their job [20]. As your practice grows, the need for flexible systems becomes even more critical, and the lack of robust remote access only worsens these challenges.
Access Limitations:
Modern behavioral health care requires flexibility and mobility.
Clinicians need to document crisis interventions in the field, conduct telehealth sessions from home, and access patient records across multiple locations. Systems without reliable cloud-based or mobile access create barriers for staff, reducing their efficiency and limiting care delivery.
69% of providers report significant interoperability issues between their EHR and other systems [14], and poor remote access only adds to these frustrations. Non-integrated telehealth tools force manual data entry, increasing the risk of errors.
"A solo LCSW in rural Maine who sees 40% of clients virtually shouldn't pay a separate monthly fee for a third-party video tool that doesn't integrate with scheduling or notes." – PIMSY Team [6]
The absence of strong remote access capabilities not only wastes clinical time but also adds to administrative burdens. Patients, too, expect digital conveniences like online intake forms, secure messaging, and mobile-friendly portals - features that are standard in other industries but are often missing in behavioral health EMRs [14][3].
The cost of limited access goes beyond daily inefficiencies. Expanding across state lines requires systems that can manage varying Medicaid billing rules and meet 42 CFR Part 2 privacy requirements for substance use records [3]. Without this adaptability, every new location becomes a compliance challenge rather than an opportunity for growth.
How to Avoid These Red Flags
Selecting the right system begins with understanding your needs and asking targeted questions before committing. With only 38% of healthcare organizations reporting that their EHR implementation met their expectations [9], taking the time for a thorough evaluation is absolutely necessary. Focus on the features that are essential for your practice and test vendors using scenarios that reflect your day-to-day operations.
Required Features to Look For
To steer clear of potential pitfalls, prioritize these essential features when evaluating an EMR system. For behavioral health practices, clinical documentation tools should be tailored for 45–60 minute sessions.
Templates need to align with behavioral health workflows, offering formats like SOAP, DAP, BIRP, and EMDR that match how clinicians work [21][6]. Treatment planning tools should allow tracking of goals and objectives over time and support collaboration across multidisciplinary teams, such as therapists, prescribers, and case managers, all on a single platform [4][6].
Compliance is another critical area. The system must include support for 42 CFR Part 2, which ensures proper handling of sensitive data. This means patient-level consent controls should be built in [5][6]. Look for ONC Certification to guarantee the platform meets federal standards for security and interoperability, a requirement for Medicare and Medicaid billing [6][10]. Additionally, role-based access controls should restrict administrative staff from accessing sensitive therapy notes [10][4].
Integration capabilities are just as important. Built-in Revenue Cycle Management (RCM) should streamline processes like real-time insurance verification, automated charge capture, and clean claim submission without requiring external tools [5][7]. Telehealth features should integrate seamlessly with scheduling and documentation workflows to avoid disruptions [5][6]. For interoperability, ensure the system supports FHIR-based data exchange and complies with the ONC's TEFCA rule, which facilitates record sharing with primary care providers for co-occurring conditions [5].
|
Feature Category |
Must-Have Attribute |
Why It Matters |
|---|---|---|
|
Clinical |
Customizable BH Templates (SOAP, DAP, BIRP) |
Reduces workflow inefficiencies, potentially saving up to 90 minutes per day [6] |
|
Compliance |
42 CFR Part 2 Support |
Ensures proper handling of sensitive substance use disorder treatment data [5] |
|
Scalability |
Multi-location Scheduling |
Supports growth and expansion to new physical locations [6] |
|
Interoperability |
ONC Certification |
Essential for Medicare/Medicaid billing and meeting federal standards [6] |
|
Engagement |
Integrated Patient Portal |
Reduces no-shows and simplifies the patient intake process [6] |
Clinical decision support and Measurement-Based Care (MBC) tools are also crucial. These tools help track patient progress and demonstrate treatment outcomes. Regulatory bodies like the Joint Commission now require standardized assessments like PHQ-9 and GAD-7 to monitor outcomes in real time [5][4]. Choose systems that automatically score these assessments and integrate results into progress notes [5][21]. For practices planning to grow, ensure the platform can scale to include more prescribers, support higher levels of care like Intensive Outpatient Programs (IOP) or Partial Hospitalization Programs (PHP), and expand across multiple locations [6].
How to Evaluate Vendors
Once you've identified the features you need, evaluate vendors systematically to ensure they can deliver. Standard demos often fall short of reflecting real-world performance. Instead, request scenario-based demos that replicate your actual workflows. For example, ask vendors to demonstrate a new patient intake, group therapy session logging, or an authorization management screen [5][6]. Pay attention to the "click count" - track how many clicks it takes to complete common tasks like starting a telehealth session or processing a medication refill. Too many clicks can waste valuable time [6].
"Investing in an EHR for your practice is more important than marketing for new clients or preparing your office space." – Kristin Trick, MA, LPC-S, RPT [10]
Ask for a detailed breakdown of the Total Cost of Ownership (TCO), including implementation fees, data migration costs, training expenses, and per-user or per-feature pricing [1]. Be sure to clarify additional costs, such as telehealth or third-party tool fees, which can significantly increase annual costs [10][6][1]. It's also important to discuss data portability - ask vendors how your data will be provided and how long it will take to retrieve it if you decide to switch systems [5].
Test the vendor's support responsiveness during your evaluation. Reach out to their support team via phone or email and assess their response times and technical expertise [1]. Confirm that support is US-based and available 24/7 for urgent clinical or billing issues [6][1]. Additionally, request references from at least three behavioral health practices similar to yours to verify the vendor's claims about implementation success and ongoing support [5][10].
Don't overlook accessibility and security. During trial periods, test the system on various devices, including phones, tablets, and desktops, to see which works best for your team and patients [10]. Ensure the system includes multi-factor authentication (MFA) for all user logins and is hosted on secure cloud platforms like Microsoft Azure to safeguard your data [6][9][1]. Finally, verify that the system maintains detailed audit trails, logging every access or change to a record - an essential feature for compliance reviews and security audits [10][4].
Conclusion
Choosing the right behavioral health EMR is a critical step in protecting your practice from costly errors that can harm patient care and overwhelm your team. The warning signs we’ve discussed - like limited customization, poor integration, weak compliance features, lack of outcome tools, and scalability issues - can severely disrupt your operations if overlooked.
The stakes are high. Consider this: EHR inefficiencies can extend workdays by an extra 90 minutes, create data silos that slow down billing, and leave your practice vulnerable to legal risks due to compliance gaps. With 75% of physicians identifying their EHR as a major factor in burnout [6], and 1 in 5 adults in the U.S. living with a mental illness [10], it’s clear that your EMR system must enhance care delivery, not obstruct it.
To steer clear of these challenges, a careful and thorough evaluation process is a must. Focus on systems with behavioral health-specific templates, built-in compliance for 42 CFR Part 2, integrated Revenue Cycle Management, and tools for Measurement-Based Care. Test potential vendors with scenario-based demos, calculate the full Total Cost of Ownership, and involve both clinical and administrative staff in the decision-making process. This approach ensures you select an EMR that supports your practice’s goals and avoids the common pitfalls that derail so many organizations.
FAQs
How do I test if an EMR fits our behavioral health workflows?
To determine whether an EMR suits your behavioral health workflows, it's crucial to assess its clinical features, flexibility for customization, and ability to support essential tasks like group therapy and treatment planning. Pay close attention to its interoperability with other systems, adherence to behavioral health regulations, and user-friendliness. Take advantage of demos or trials to explore these aspects firsthand. Additionally, testing automation tools can help confirm data accuracy and security. Hands-on testing is key to ensuring the system meets your unique requirements.
What integrations should a behavioral health EMR have from day one?
A behavioral health EMR should come equipped with telehealth platform integrations, clinical decision support tools, care coordination features, and interoperability with other health systems. These components work together to streamline data sharing and promote well-rounded patient care from the very beginning.
Which compliance features are must-haves for 42 CFR Part 2 and HIPAA?
To meet the privacy and security standards required for behavioral health, your EMR should include the following essential features:
Granular consent management: This allows patients to specify who can access their Substance Use Disorder (SUD) records and for what purpose.
Flagging and restricting re-disclosure: Ensures that SUD records are not shared without proper authorization, maintaining strict confidentiality.
Audit trails: Tracks and logs all disclosures, providing a transparent record of who accessed sensitive information and when.
Encryption: Protects patient data by securing it during storage and transmission.
Role-based access controls: Limits access to sensitive records based on a user's role, ensuring that only authorized personnel can view or modify data.
Breach notification adherence: Ensures compliance with regulations requiring timely notification in the event of any data breach.
These features are critical to ensuring your EMR system aligns with the privacy and security requirements of both 42 CFR Part 2 and HIPAA.
