Behavioral health risk assessment frameworks are structured methods for evaluating risks like self-harm, harm to others, or victimization.
These frameworks rely on evidence-based tools and clinical expertise to improve safety and guide treatment decisions. They typically involve five stages: identifying risks, analyzing them, creating action plans, implementing treatments, and ongoing monitoring.
Key benefits include:
Improved safety: Helps clinicians identify and manage risks effectively.
Better treatment outcomes: Supports accurate diagnoses and personalized care.
Regulatory compliance: Ensures facilities meet standards for accreditation and funding.Frameworks like the ASAM Criteria, used in addiction treatment, assess multiple aspects of a patient's life to determine the right care level. Tools like the Columbia-Suicide Severity Rating Scale (C-SSRS) and Ask Suicide-Screening Questions (ASQ) play a vital role in assessing risks and tailoring interventions.
Modern Electronic Health Record (EHR) systems enhance these processes by automating tasks, reducing errors, and improving documentation. These systems allow clinicians to focus more on patient care while meeting compliance requirements.
Why Behavioral Health Facilities Use Risk Assessment Frameworks
Behavioral health facilities depend on risk assessment frameworks for three main reasons: ensuring patient safety, enhancing treatment outcomes, and meeting regulatory standards. These priorities guide every step of the framework process, from identifying risks to ongoing monitoring.
Patient safety is a major driver for using these frameworks because risks in behavioral health can change rapidly and escalate without warning. A structured approach allows staff to spot potential hazards, evaluate the likelihood of violence, and keep risks under control [3][4]. As the Royal College of Psychiatrists explains:
"Risk cannot be eliminated, but it can be rigorously assessed and managed or mitigated" [4].
This focus on safety has even influenced legislation, such as a 2022 law in Louisiana aimed at addressing workplace violence in healthcare settings [3].
Improved treatment outcomes are another critical advantage. By documenting risks, clinicians can make more accurate diagnoses and create tailored treatment plans [1].
These frameworks not only identify potential dangers but also emphasize protective factors - like a patient’s coping mechanisms, social networks, and reasons for living - that are essential for building personalized safety plans [1]. With nearly 1 in 5 U.S. adults diagnosed with a mental health condition as of 2019, these structured systems help care teams adapt interventions as patients’ needs change over time [6].
Regulatory compliance is also a key consideration. Facilities must align their risk assessment and documentation practices with recognized frameworks to qualify for reimbursements and pass accreditation reviews from organizations like The Joint Commission or CARF [2]. Falling short of these standards could cost a facility as much as $14 million [8].
Healthcare Compliance Pros highlights the value of these frameworks in maintaining compliance, stating:
"It minimizes risk, sustains patient trust, and meets regulatory standards" [7].
What Makes Up a Behavioral Health Risk Assessment
Behavioral health risk assessments bring together data collection, evaluation methods, and tailored action plans. These elements work together to help clinicians understand a patient's risk level and decide on the best steps to ensure their safety.
Collecting Patient Data and Information
Risk assessments pull information from multiple areas: clinical, psychological, environmental, and protective factors. Clinicians document critical details such as suicidal thoughts, planning, access to means, and any history of self-harm or violence.
They also assess behaviors and emotions like impulsivity, mood swings, feelings of hopelessness, aggression, trauma, and signs of psychosis. Environmental factors like life stressors, social isolation, and the patient's support system are also taken into account. On the other hand, protective factors - such as coping skills, personal strengths, and reasons to live - play a key role in balancing the risk picture [1].
Accurate and thorough documentation is essential. Not only does it guide clinical care, but it also serves as a legal record of the provided care. For telehealth assessments, clinicians are encouraged to confirm the patient’s physical location at the start of each session and keep an emergency contact on file.
Once all the necessary data is collected, clinicians use a mix of professional judgment and validated tools to evaluate the risks.
Models for Evaluating Risk
Risk evaluation blends subjective inputs - like patient self-reports and personal perceptions - with objective data, such as measurable symptoms and cognitive markers [9].
Modern approaches balance clinical expertise with established tools like the PHQ-9 for depression or the C-SSRS for assessing suicide risk. Risk is not static; it requires regular reassessment [4].
For example, Denver Health launched an EHR data integration project between July 2021 and February 2022 to standardize tracking for substance use disorder (SUD) treatment. After full implementation, the number of patients tracked for SUD treatment initiation jumped from 562 to 1,411 - a 250% increase [10].
Physical health should also be evaluated during risk assessments. Conditions like thyroid disorders or vitamin deficiencies can mimic mental health issues, leading to misdiagnosis. This is especially important given the high rates of misdiagnosis: 65.9% for major depressive disorder, 92.7% for bipolar disorder, and 71.0% for generalized anxiety disorder [9].
The insights from these evaluations lay the groundwork for action plans tailored to address the identified risks.
Creating Action Plans from Assessment Results
Using the findings from risk evaluations, clinicians craft specific, patient-focused action plans. These plans often include two parts: safety plans for immediate guidance between sessions and treatment plans for managing symptoms over time.
Collaboration with the patient is key, ensuring the plan includes clear elements like warning signs, coping strategies, social support networks, emergency contacts, and ways to limit access to lethal means.
The Los Angeles County Psychological Association highlights the importance of documentation:
"Preparing and maintaining clinical notes provides evidence of the standard of care and that the risk of legal or ethical violations has been managed." [1]
Action plans align specific risks with appropriate interventions. For example, stabilization efforts, safety measures, or evidence-based treatments like Dialectical Behavior Therapy (DBT) and Cognitive Behavioral Therapy (CBT) may be recommended.
Community resources - such as support groups, religious organizations, or 12-step programs - can also be integrated. For high-risk patients, the plan might include transitioning to more intensive care, such as hospitalization when necessary [11].
Standard Tools and Instruments for Risk Assessment
Standardized tools have become essential for consistent and reliable risk measurement, complementing tailored patient action plans.
Among these, the Columbia-Suicide Severity Rating Scale (C-SSRS) is widely recognized as a key instrument for assessing suicide risk. In 2012, the FDA identified it as the standard for evaluating suicidal ideation and behavior in clinical trials [16].
The C-SSRS uses straightforward questions to assess a range of risks, from a simple "wish to be dead" to "active suicidal ideation with a specific plan and intent" [13]. Notably, individuals exhibiting identified suicidal behavior are 8 to 10 times more likely to die by suicide [13].
Another important tool is the Ask Suicide-Screening Questions (ASQ), which focuses on pediatric medical patients. Research shows that nearly 50% of individuals who die by suicide had visited a healthcare provider within the month before their death.
Alarmingly, clinicians screening only for depression may miss suicide risk in about 33% of their patients [17]. Below, we explore how these tools are implemented in practice and examine their strengths and limitations.
How Each Tool Is Used in Practice
The C-SSRS offers different versions tailored to various clinical settings. For example:
Screener version: With just 2 to 6 questions, it's ideal for quick assessments in fast-paced environments like emergency rooms.
Full scale: Provides a detailed evaluation of both suicidal ideation and behavior.
Healthcare providers often use the "Lifetime/Recent" version during initial assessments and the "Since Last Visit" version for follow-ups [17].
Dr. Kelly Posner Gerstenhaber, Founder and Director of The Columbia Lighthouse Project, underscores the tool's purpose:
"It's about saving lives and directing limited resources to the people who actually need them" [16].
The C-SSRS is designed for both clinical and non-clinical users. It incorporates caregiver input and patient records to complement self-reported data [13][16][17].
Organizations often use specific criteria based on "yes/no" responses. For instance, patients reporting ideation levels of 4 or 5 within the past month are flagged for immediate, comprehensive risk assessments by licensed mental health professionals [16][17].
The tool is also available in over 150 languages and is free for use in community, healthcare, and nonprofit research settings [16][12]. These practical applications highlight its versatility in real-world scenarios.
What Each Tool Does Well and Where It Falls Short
Understanding the strengths and limitations of these tools is essential for improving patient care and meeting compliance requirements. The C-SSRS is particularly effective at capturing a broad spectrum of suicidal thoughts and behaviors.
It evaluates four key types of suicidal behavior - actual attempts, interrupted attempts, aborted attempts, and preparatory actions (e.g., purchasing a weapon or writing a note) [13][16].
Its conversational style and plain language make it accessible to non-clinicians, broadening its usability beyond traditional mental health settings. Additionally, it provides detailed data on severity, frequency, duration, and lethality, which is invaluable for treatment planning [17].
However, while the C-SSRS offers critical insights, clinical judgment remains indispensable. Patient responses must be interpreted within the larger context of their personal history, current stressors, and protective factors.
Modern behavioral health EHR systems enhance these tools by automating documentation, integrating multiple assessments, and ensuring compliance with standards set by organizations like the Joint Commission or CARF [14][15].
The 4 Stages of Risk Assessment
4 Stages of Behavioral Health Risk Assessment Framework
Risk assessment in behavioral health involves a step-by-step process designed to transform collected data into actionable treatment plans. Each phase builds upon the previous one, addressing both immediate safety needs and ongoing care requirements.
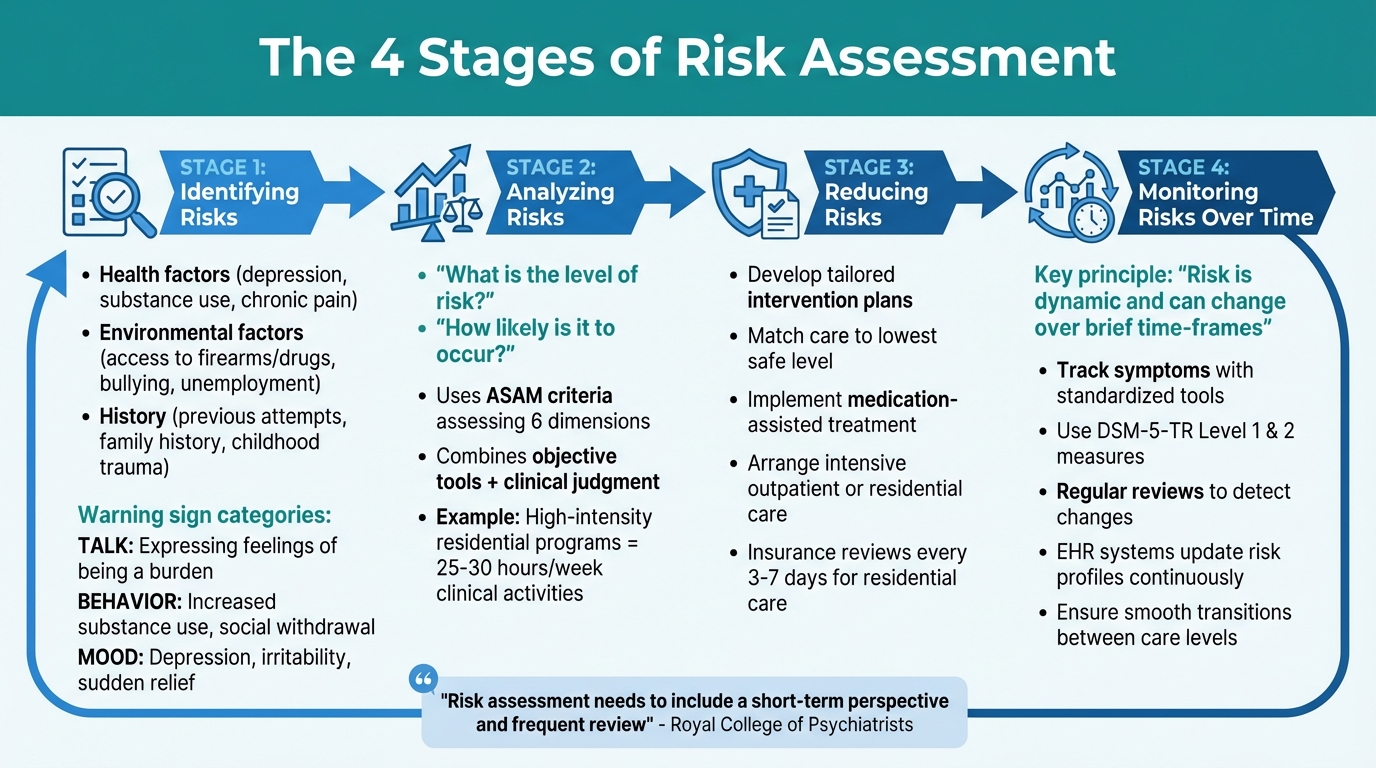
Stage 1: Identifying Risks
This stage is all about collecting information to establish a clear picture of potential risks and protective factors. Clinicians consider a range of factors, including:
Health: Mental health conditions like depression, substance use disorders, or chronic pain.
Environment: Access to firearms or drugs, bullying, unemployment.
History: Previous suicide attempts, family history of suicide, or childhood trauma [19].The SAFE-T framework (Suicide Assessment Five-Step Evaluation and Triage) highlights this step as essential for understanding risks and protective elements [18].
According to the GPMHSC:
"A risk assessment is a direct conversation with a patient about their suicidal thoughts, plans and intent; it is a matter-of-fact empathetic conversation that allows patients to discuss suicide openly." [20]
Clinicians also look for warning signs in three main categories: Talk (expressing feelings of being a burden or having no reason to live), Behavior (increased substance use, social withdrawal, or giving away possessions), and Mood (depression, irritability, or sudden relief) [19].
For children and adolescents, input from parents, teachers, and the youth themselves enhances the accuracy of risk identification [21]. Electronic Health Record (EHR) systems further support this process by distributing targeted screening tools [5].
Stage 2: Analyzing Risks
Once risks are identified, the next step is to evaluate their severity and likelihood. This stage focuses on answering two key questions: "What is the level of risk?" and "How likely is it to occur?" [1]. This analysis helps prioritize interventions and allocate resources effectively [22].
In treating substance use disorders, many states rely on the ASAM (American Society of Addiction Medicine) criteria to guide placement decisions [2].
These criteria assess patients across six dimensions, such as withdrawal potential and living environment, to recommend the appropriate level of care. For example, patients in high-intensity residential programs (Level 3.5) typically engage in 25–30 hours of clinical activities weekly [2].
The American Psychiatric Association highlights the value of this documentation:
"Documenting an estimation of a patient's suicide risk may improve a clinician's decision-making about the patient's diagnosis and treatment plan." [1]
Objective tools work alongside clinical judgment to provide a comprehensive risk analysis. For instance, a patient with moderate mental health challenges and a difficult home environment may require higher prioritization than someone with severe symptoms in only one area [2].
Stage 3: Reducing Risks
This phase focuses on turning the analysis into actionable steps to lower the identified risks. Clinicians develop a tailored plan that addresses both immediate concerns and long-term needs [18][4].
Interventions are matched to the patient’s specific risk profile, ensuring care is delivered at the lowest level that can safely meet their needs [2].
Strategies for reducing risks vary depending on the situation. For substance use disorders, options might include medication-assisted treatment, intensive outpatient programs, or residential care. Insurance providers often review residential care every 3–7 days to ensure continued treatment is justified based on updated risk assessments [2].
Proper documentation is crucial here, especially when explaining why a particular level of care is necessary and why a less intensive option wouldn’t suffice [2].
Stage 4: Monitoring Risks Over Time
The final stage acknowledges that risk levels can fluctuate. As the Royal College of Psychiatrists notes:
"Risk is dynamic and can be affected by circumstances that can change over the briefest of time-frames. Therefore, risk assessment needs to include a short-term perspective and frequent review." [4]
Ongoing monitoring involves tracking symptoms and patient-reported outcomes using standardized tools. The American Psychiatric Association has developed DSM-5-TR Level 1 and Level 2 cross-cutting measures for this purpose:
"These patient assessment measures were developed to be administered at the initial patient interview and to monitor treatment progress, thus serving to advance the use of initial symptomatic status and patient reported outcome (PRO) information." [23]
Regular reviews help detect changes in a patient’s risk level, whether it’s increasing or decreasing [4]. EHR systems continually update risk profiles, ensuring treatment plans remain aligned with the patient’s evolving needs [5].
This approach supports smooth transitions between care levels and ensures interventions stay relevant as circumstances shift [4]. It also sets the stage for leveraging EHR systems to streamline documentation and improve patient care, which will be explored in the next section.
Using EHR Systems to Support Risk Assessments
EHR systems simplify the risk assessment process by organizing patient data, utilizing clinical algorithms, and delivering real-time insights at every stage.
Platforms like Opus Behavioral Health EHR are designed to integrate seamlessly into the workflow, from identifying risks to continuous monitoring. These tools are especially tailored to meet the documentation and compliance needs of behavioral health and addiction treatment facilities.
Automating Risk Assessment Tasks
Automation within EHR systems reduces errors and speeds up the risk assessment process. By pulling data from sources like intake forms, historical records, and telehealth sessions, these systems automatically populate standardized templates and risk checklists with relevant details such as prior assessments and vital signs [28][29].
Built-in algorithms then score risks and flag potential high-risk indicators in real time.
For example, Opus Behavioral Health EHR uses AI-powered tools to process outcomes measurement data, cutting manual data entry errors by up to 70% and allowing clinicians to complete assessments 40% faster [28][29].
Its Copilot AI feature even captures and organizes clinical notes during patient visits [24][25]. Judd Carey, Director of Operations at VirtualServices, Mindful Health, highlights the importance of this automation:
"By automating the quality of internal data, and applying an algorithm, it will cut back on errors to not miss a thing, especially from group sessions." [25]
Automation supports every stage of risk assessment.
For instance:
Checklists are auto-populated during the identification phase.
Rule-based scoring is applied during analysis.
Tailored action plans, including e-prescribing links, are generated for risk reduction.
Follow-ups are scheduled with automated alerts for ongoing monitoring [26][27].This efficiency translates into significant time savings. One behavioral health center reported cutting reassessment times from days to hours and reducing documentation discrepancies by 50% after implementing automated analysis for substance use disorder risk models [27][28].
Better Documentation and Reporting
EHR systems improve documentation and reporting by enforcing standardized templates and creating HIPAA-compliant audit trails with timestamped entries.
Real-time dashboards compile assessment data into instant reports, while automated quality control ensures no critical information is overlooked. For example, Opus Behavioral Health EHR offers over 140 reports that align with SAMHSA requirements and Joint Commission standards, exporting compliance-ready documents [29][30].
The platform also links billing directly to assessment outcomes through built-in RCM tools, helping facilities achieve a 99% audit pass rate in reported implementations [26][31].
Centralized data access enables psychiatrists, therapists, and case managers to view risk reports simultaneously through role-based portals, eliminating redundant data entry. CRM integration ensures teams are notified immediately when risk levels change.
Amanda Wilson, Director of Clinical Services at a Mental Health and Substance Use Treatment Center, emphasizes the operational benefits:
"This process will simplify our operations to save so much time. We will no longer have to manually pull so many charts per quarter and have a timelier billing process for quicker reimbursements." [25]
Additionally, integrated lab modules allow providers to order and receive test results directly within the EHR, ensuring diagnostic data is accurately reflected in the patient's risk profile without manual errors [25].
By streamlining documentation, these systems enable more precise and timely interventions based on reliable data.
Supporting Better Patient Care
EHR systems empower better decision-making by analyzing aggregated data from multiple assessments to generate predictive insights. They link treatment adherence to risk reductions, producing metrics like relapse probability scores that guide personalized care plans.
Facilities using Opus Behavioral Health EHR have reported 25–35% improvements in retention rates for substance use disorder programs through these targeted interventions [28][30].
Real-time alerts enhance patient safety by continuously monitoring vital signs, lab results, and clinical notes to identify warning signs early - sometimes hours before a crisis [25].
Patient engagement tools further support care by allowing individuals to self-report crisis symptoms, which are immediately shared with care teams for proactive adjustments to treatment. One addiction treatment center reduced readmissions by 40% using automated risk monitoring integrated with telehealth [29][32].
Another facility boosted recovery rates by 28% by using EHR analytics to identify at-risk groups for targeted interventions [29][32].
By reducing administrative burdens, AI-powered tools give clinicians more time to focus on patient care. Providers using behavioral health-specific EHRs report spending 35% less time on documentation while capturing more detailed clinical data [24].
Dr. Jennifer Williams, a Mental Health Practice Owner, shares:
"Since implementing Opus EHR, our providers spend 35% less time on documentation while capturing more comprehensive clinical data." [24]
With over 100 customizable assessment tools, Opus Behavioral Health EHR simplifies outcomes measurement and uncovers clinical trends through dynamic dashboards.
This helps providers see the "complete patient story", something often missed in static charts [24]. The combination of automation, real-time monitoring, and data visualization ensures that treatment plans evolve with patients' needs, while maintaining the clinical rigor required for effective care.
Key Takeaways
Structured risk assessment frameworks transform subjective evaluations into research-driven processes, improving patient safety and clinical decision-making.
These tools help clinicians identify immediate risks, gauge severity, create personalized treatment plans, and maintain thorough documentation to protect providers. As the American Psychiatric Association highlights:
"documenting an estimation of a patient's suicide risk may improve a clinician's decision-making about the patient's diagnosis and treatment plan" [1].
This foundation paves the way for digital tools that further improve compliance and operational efficiency.
Opus Behavioral Health EHR streamlines these frameworks by automating data collection, reducing transcription errors, and flagging risks in real time. Digital intake systems allow patients to input information directly into the EHR, encouraging more honest disclosures on sensitive topics. Plus, mandatory field logic ensures records are complete [33].
These features not only enhance data accuracy but also simplify compliance with regulatory requirements.
The benefits of specialized behavioral health EHRs are tangible. For example, facilities using automated systems often cut audit preparation time by 50% or more while staying aligned with CARF, Joint Commission, and state regulations.
Mira Gwehn Revilla explains:
"digital intake acts as a 'truth filter' for addiction treatment documentation. The result is cleaner clinical records that hold up during CARF, Joint Commission, and state audits" [33].
These advancements help facilities maintain high clinical and regulatory standards.
Risk assessment also demands ongoing updates as patient conditions evolve.
The American Psychological Association stresses:
"assessment competence is not static, but requires ongoing, deliberate effort" [1].
Platforms like Opus Behavioral Health EHR support this need with automated alerts and standardized documentation, reinforcing a commitment to dynamic and responsive patient care [33].
FAQs
How often should risk assessments be repeated?
Risk assessments need to be conducted regularly and revisited whenever there are major changes in someone's situation or surroundings.
How often this happens depends on the context, the purpose of the assessment, and the risks at play. By reassessing on a consistent basis, you can quickly spot and manage any new or shifting risks.
When do screening tools trigger urgent action?
Screening tools play a crucial role in identifying serious safety concerns, such as suicidal thoughts, self-harm behaviors, or situations where someone may pose an immediate risk to themselves or others. When these red flags are detected, they demand swift evaluation and prioritization to ensure safety and connect individuals with the care they urgently need.
How can an EHR improve risk assessment accuracy?
An Electronic Health Record (EHR) improves the accuracy of risk assessments by offering real-time clinical data and utilizing AI-driven tools. Platforms like Opus Behavioral Health EHR ensure patient records are complete and current, which helps reduce overlooked risk factors.
With AI-assisted documentation, errors decrease, while customizable workflows and templates allow assessments to be adapted to individual patient needs. These capabilities simplify data analysis, giving clinicians more time to concentrate on providing accurate and dependable behavioral health evaluations.
