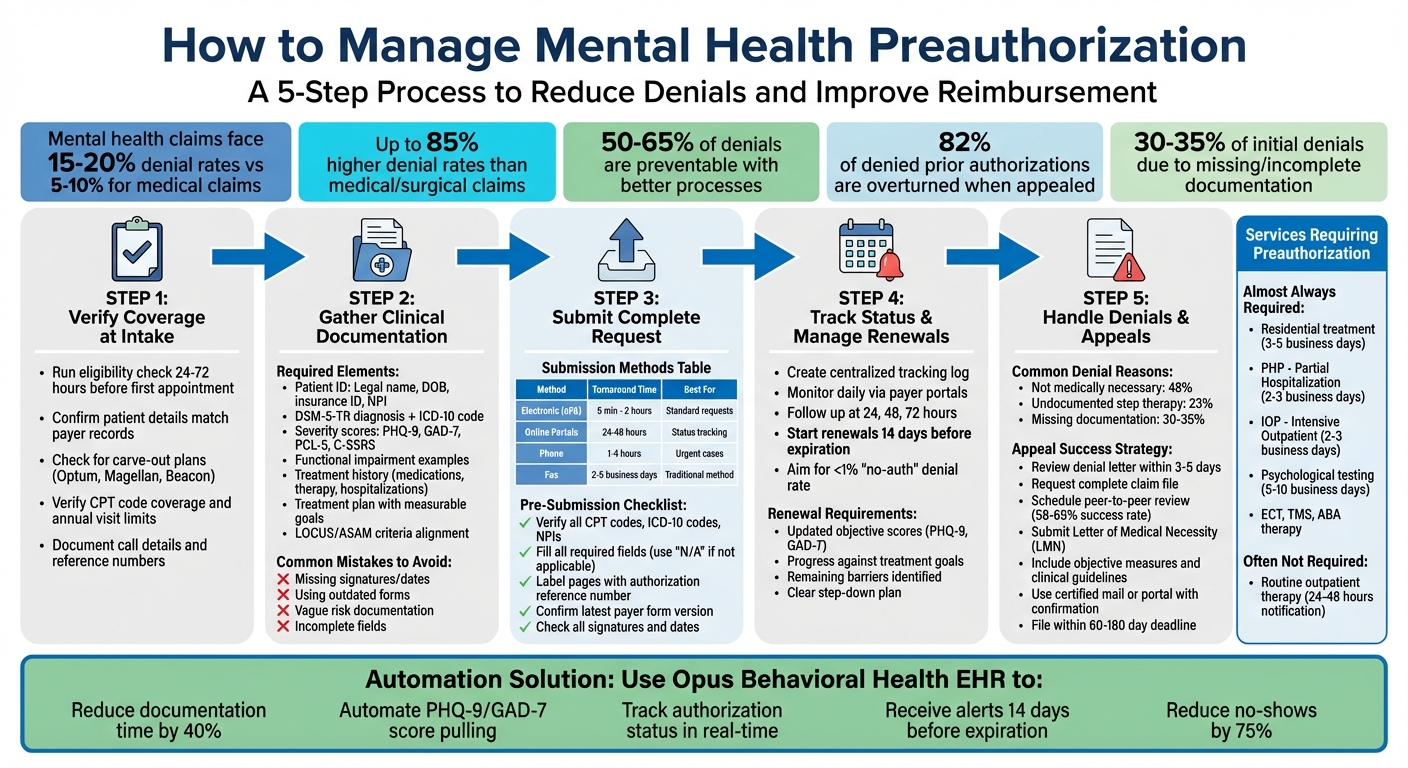
Mental health providers face high denial rates - up to 85% more than medical claims - due to complex and fragmented preauthorization processes.
Without proper preauthorization, claims are often denied, leading to financial losses and disrupted patient care.
This guide simplifies the process with actionable steps to reduce denials, save time, and improve reimbursement outcomes.
Here's what you'll learn:
Understand payer rules: Know which services need preauthorization and the required documentation.
Verify coverage early: Confirm insurance details during patient intake to avoid errors.
Prepare complete documentation: Include DSM-5 diagnoses, severity scores (e.g., PHQ-9), and treatment history.
Submit requests accurately: Use correct submission methods, like electronic portals, for faster approvals.
Track and renew authorizations: Monitor statuses and start renewals 14 days before expiration.
Appeal denials effectively: Most denials can be overturned with clear, detailed appeals.
5-Step Mental Health Preauthorization Process to Reduce Claim Denials
Know Your Payer's Preauthorization Rules
To cut down on preauthorization headaches and avoid denials, it's essential to understand the rules set by each payer.
Insurers have specific guidelines about which services need approval, how to submit requests, and what documentation is required. Knowing these details upfront can save time and prevent errors that lead to delays or outright denials.
1. Find and Review Payer Guidelines
Start by accessing each insurer's secure portal. Many major insurers, like Optum's Provider Express or Molina's Availity portal, allow you to check service-specific authorization requirements by entering the patient's member details and the relevant CPT code[5][9]. Some insurers also offer public "Prior Authorization LookUp Tools" for quick checks.
If online tools don’t provide clear answers, reach out to the payer's authorization department. Have the patient's ID, date of birth, and procedure codes ready. Request verbal confirmation and ask for documentation requirements via email or fax [8].
Cross-check service-specific requirements using both provider portals and the patient’s Summary of Benefits and Coverage (SBC). Additionally, many insurers publish clinical criteria manuals - like ASAM for addiction or LOCUS for mental health - on their websites to explain the medical necessity standards they use [1][9].
To stay organized, create an authorization matrix for your practice.
This can be a spreadsheet listing high-volume services (e.g., 90837, IOP, PHP), whether preauthorization is needed for each payer, typical authorization timeframes, and required documents [1].
Make sure to date-stamp entries and assign someone to keep it updated. This tool helps avoid outdated information and reduces the risk of same-day cancellations or denials due to missing authorizations [1][8].
Check if your practice qualifies for programs like UnitedHealthcare's Gold Card, which simplifies preauthorization for providers with strong performance metrics [3][9].
Once you’ve reviewed these guidelines, you’ll be ready to confirm coverage requirements during patient intake.
2. Typical Requirements for Behavioral Health Services
For behavioral health services, most payers require specific clinical and administrative information.
This often includes a DSM-5 diagnosis, severity scores (e.g., PHQ-9,GAD-7), and a risk or safety assessment.
You’ll also need to show that the requested level of care is medically necessary, using frameworks like the ASAM Criteria for substance use disorders or tools like InterQual, Milliman, and LOCUS/CALOCUS for mental health services.
Treatment plans should outline measurable goals, evidence of progress, and reasons for stepping up care.
For higher levels of care, such as Residential or Partial Hospitalization Programs (PHP), it’s crucial to document prior lower-intensity treatments to justify the need for escalation.
Administrative details like CPT codes, requested units or sessions, provider NPI, and patient insurance information must also be included [8]. A complete preauthorization request combines these clinical and administrative elements.
Services that typically require preauthorization include:
Residential treatment
Partial Hospitalization Programs (PHP)
Intensive Outpatient Programs (IOP)
Psychological and neuropsychological testing
Medication-Assisted Treatment (MAT) for certain medications
Electroconvulsive Therapy (ECT)
Transcranial Magnetic Stimulation (TMS)
Applied Behavior Analysis (ABA)
Extended outpatient therapy beyond a set number of sessionsRoutine outpatient therapy often doesn’t need preauthorization or may only require notification.
However, some payers limit the number of visits they authorize at a time, which can lead to ongoing reauthorization cycles for continued therapy [4].
|
Service Category |
Typical PA Requirement |
Standard Turnaround Time |
|---|---|---|
|
Routine Outpatient Therapy |
Often Not Required (or Notification only) |
24–48 hours |
|
Intensive Outpatient (IOP) |
Almost Always Required |
2–3 business days |
|
Partial Hospitalization (PHP) |
Almost Always Required |
2–3 business days |
|
Residential Treatment |
Always Required |
3–5 business days |
|
Psychological Testing |
Frequently Required |
5–10 business days |
To streamline the process, standardize clinical packets to include necessary scores, a rationale for the level of care, and a record of previously attempted lower-intensity treatments [1].
This reduces the chances of denials due to missing information and can help speed up approvals.
Also, for urgent care requests, keep in mind that state laws often require insurers to respond within 24 to 72 hours, while non-urgent requests may take up to 15 days, depending on the state [3][8].
Step 1: Verify Coverage and Service Requirements at Intake
Getting insurance details right from the start can help you sidestep most preauthorization headaches.
By confirming coverage early, you can pinpoint which services need approval, understand submission timelines, and ensure the patient's plan is active. This sets the stage for a smoother revenue cycle.
Check Insurance Eligibility and Benefit Limits
Run an eligibility check 24–72 hours before the patient’s first appointment.
This step helps you catch issues like inactive coverage or carve-out plans, where behavioral health benefits are handled by a third-party administrator (e.g., Optum, Magellan, or Beacon) [10].
Make sure the patient’s name, date of birth, member ID, and group number match the payer's records exactly. Double-check that the policy is active by reviewing the effective and termination dates - this prevents claims from being filed during coverage gaps.
Ask about coverage for specific CPT codes. For instance, some plans may cover 45-minute sessions without preauthorization but require approval for 60-minute sessions (CPT 90837).
Identify annual visit limits, track sessions already used, and confirm details like remaining deductibles, copays, coinsurance, and out-of-pocket maximums. Also, ensure that both the facility's and provider's NPIs are in-network.
Document every call thoroughly, including the insurance representative’s name, the call date, and the reference number.
"A single oversight - like missing a visit limit or not confirming authorization requirements - can delay or deny payment, burden the patient with unexpected costs, and erode trust in your practice." - Aarogram Team [10]
After verifying coverage and benefits, you’ll know which services specifically require preauthorization.
Identify Which Services Need Preauthorization
Once you’ve confirmed coverage, shift your focus to identifying services that need preauthorization. Cross-check planned services against your payer-service matrix - a spreadsheet that outlines authorization requirements for high-volume services like Intensive Outpatient Programs (IOP), Partial Hospitalization Programs (PHP), and CPT 90837 [1].
If the matrix doesn’t provide a clear answer, contact the payer’s authorization department with the patient’s ID, date of birth, and specific CPT codes to confirm what’s required [10].
"Front‑office/billing teams must ask about specific CPT coverage during eligibility checks. This is critical because some plans exclude longer sessions or place limits on psychotherapy combined with E/M." - Aarogram Team [10]
Also, check for eligibility in programs like UnitedHealthcare's Gold Card, which waives prior authorization for certain providers and procedure codes, requiring only advance notification.
For telehealth services, confirm that the patient’s plan includes virtual visits and verify necessary modifiers (e.g., 95, GT) and the correct Place of Service (POS) code (e.g., 10 for home).
Since prior authorization requests typically take 3 to 5 business days to process [8], identifying requirements during intake can help avoid delays in starting essential treatments.
Step 2: Gather Required Clinical Documentation
Once you've confirmed coverage and service requirements during intake, the next step is to ensure all clinical documentation is accurate and complete.
This is critical for securing preauthorization. Mental health and substance use disorder claims face denial rates that are up to 85% higher than medical and surgical claims [2]. Missing or incomplete documentation contributes to 30–35% of initial denials [14]. The good news? Most of these denials can be avoided by organizing the necessary paperwork upfront.
Collect Patient and Treatment Information
Start with the basics: gather the patient’s legal name, date of birth, insurance ID, group number, and the provider's NPI [11][8].
Surprisingly, 50% of denied insurance claims stem from insufficient patient identification [12]. To avoid this, double-check that all identifying details are accurate.
Next, include the DSM-5-TR diagnosis along with its corresponding ICD-10 code. Be specific - vague or generalized diagnoses won’t cut it [2][11]. For example, include objective scores like PHQ-9, GAD-7, PCL-5, or C-SSRS to support the diagnosis [2][1].
When documenting functional impairment, use measurable examples. Instead of writing "patient is depressed", specify something like "patient missed 12 days of work in the past month" or "unable to care for children without assistance" [2].
Tools like Global Assessment of Functioning (GAF) or WHODAS 2.0 can also help quantify how the condition affects key areas like work, relationships, and daily life [2].
Your documentation should also outline the patient’s treatment history. Include details about previous medications (dosages and duration), therapy methods, hospitalizations, and the patient’s response to each [2][8][14].
Insurance providers often require evidence that less intensive treatments were attempted before approving higher levels of care. For intensive programs like IOP, PHP, or residential treatment, align your records with established frameworks such as LOCUS (Level of Care Utilization System) or ASAM criteria [2][1].
Additionally, attach an individualized treatment plan that includes therapy modalities, session frequency, measurable goals, and a clear justification for the requested level of care [11][1][8].
When all the necessary information is collected, the key is to present it in a clear and organized manner.
Avoid Common Documentation Mistakes
Even small errors can lead to denials or delays, so attention to detail is crucial. Make sure every required field is filled out - use "N/A" if something doesn’t apply [13][8].
Missing signatures or dates on clinical documents are a common reason for administrative denials, so double-check that every page is signed and dated before submission [11][13].
Also, always use the most up-to-date payer forms, which can usually be found on the insurer's provider portal [13].
When documenting risk or safety concerns, avoid vague terms like "patient is at risk." Instead, provide specific details, such as C-SSRS scores or concrete behaviors [13][1].
For renewal requests, don’t simply copy and paste the patient’s initial history. Show their current status and progress toward treatment goals to demonstrate the ongoing need for care [1].
Organize your records chronologically, and write the authorization reference number on every page. This ensures documents won’t get separated during the review process [8].
"A provider note that clearly documents the patient's functional impairment... is an authorization asset. A note that describes the same clinical picture in vague generalities is an authorization liability." - clinIQ [14]
Step 3: Submit Complete Prior Authorization Requests
Once you've collected all the necessary documentation, it's time to submit your prior authorization request with precision.
Considering that physicians handle an average of 39 requests per week [7], even a single mistake can result in a denial. The objective is clear: send a complete and error-free packet to the correct destination using the appropriate submission method.
Choose the Correct Submission Method for Each Payer
Payers have specific channels for submitting prior authorization requests, and using the wrong method can lead to delays. Common submission methods include:
Electronic Prior Authorization (ePA): The fastest option, with responses typically arriving within 5 minutes to 2 hours.
Online payer portals: Platforms like Availity allow you to upload documents and track status, usually within 24 to 48 hours.
EDI 278 transactions: Submit directly from your EHR system.
Phone calls: Ideal for urgent or expedited cases, with turnaround times of 1 to 4 hours.
Fax: A traditional method that takes 2 to 5 business days but can be harder to track [7][8].It's also crucial to check whether the payer delegates certain services to third-party vendors like eviCore or Carelon.
You can verify this by visiting their portal or contacting their authorization line [7].
Sending your request to the wrong entity wastes valuable time and increases the likelihood of denial. For elective procedures, aim to submit requests 5 to 10 business days before the scheduled service date, ensuring adequate time for processing [7].
|
Submission Method |
Typical Turnaround Time |
Best Use Case |
|---|---|---|
|
Electronic (ePA) |
5 minutes – 2 hours |
Standard non-urgent requests; most efficient |
|
Online Portals |
24 – 48 hours |
Tracking status and uploading documents |
|
Phone |
1 – 4 hours |
Urgent or expedited cases |
|
Fax |
2 – 5 business days |
Traditional method; difficult to track |
Accurate submission builds on the solid foundation of your documentation, ensuring a smooth preauthorization process.
Check and Double-Check for Accuracy
Before hitting "submit", take a moment to review every detail. A small error, like a transposed digit in a member ID or NPI, can lead to a denial [7].
Carefully cross-check all CPT codes, ICD-10 codes, NPIs, and member IDs against your source documents. Make sure every required field is filled out - even if a section doesn’t apply, write "N/A" instead of leaving it blank [13].
Additionally, label every page of supporting documents with the authorization reference number to avoid separation during processing [13].
A secondary review of the packet can catch preventable mistakes, significantly reducing the chance of denials.
"Incomplete documentation causes delays and denials." - Sami Malik, Founder & CEO of Linear Health [7]
Confirm that all required signatures are present and properly dated. Also, ensure you're using the latest version of the payer's form. Some payers, like UnitedHealthcare, allow only a 3-business-day window to submit missing information before issuing a denial [7].
With your request submitted accurately, you're now ready to move on to tracking its status and managing renewals.
Step 4: Track Status and Manage Renewals
After submitting your request, the next step is to focus on tracking authorization statuses and ensuring renewals are handled on time. This phase is all about staying organized and proactive.
Monitor Request Status
Start by creating a centralized tracking log. This should include key details like the submission date, payer name, authorization reference number, and the expected decision date. Assign a dedicated Utilization Management specialist to monitor the log and oversee updates [1].
This specialist should check payer portals daily for real-time updates and make phone calls for urgent cases that require verbal confirmation.
Establish a follow-up schedule to review pending requests at regular intervals - 24, 48, and 72 hours after submission [1]. If no decision is received by Day 4 or 5, escalate the matter to a supervisor at the insurance company [8].
"Prior authorization in behavioral health doesn't need to be chaotic. With a visible payer–service matrix, reviewer-ready packets, ePA plus timers, disciplined renewals, and parity-aware appeals, mental health billing and prior auth becomes predictable and fast." - Lisa Martin, Mental Health Billing Expert, AnnexMed [1]
Once you've updated the request statuses, shift your attention to renewals, ensuring they are secured well before any authorizations expire.
Plan for Renewals Before Expiration
To avoid lapses in authorization, start the renewal process 14 days before the current authorization expires [1].
Unlike one-time surgical approvals, mental health services often require ongoing reviews. These reviews extend authorizations every few sessions and rely on updated clinical scores, such as PHQ-9 or GAD-7.
When submitting a renewal request, include the following:
Updated objective scores
Progress against measurable treatment goals
Identification of remaining barriers to treatment
A clear plan for step-down or tapering [1][4]
Top-performing behavioral health practices aim for a "no-auth" denial rate of less than 1% [1]. To achieve this, confirm receipt of the renewal request within 24 hours. If no acknowledgment is received within two weeks, follow up by phone [13][8].
Keep in mind: an approved authorization confirms medical necessity but does not guarantee payment if the patient's eligibility changes before the service date. Staying vigilant is key to ensuring smooth operations.
Step 5: Handle Denials and File Appeals
Even with careful preparation, claim denials can happen, especially for mental health services. In fact, mental health claims face denial rates of 15–20%, compared to 5–10% for medical or surgical claims [6].
The good news?
About 82% of denied prior authorizations are overturned when appealed [18]. Yet, surprisingly, fewer than 1% of providers file appeals, leaving potential revenue and patient care unaddressed [17].
Review Denial Reasons
Start by reviewing the denial letter within 3–5 business days [15]. Pay close attention to the reason code and clinical criteria the payer used to justify the denial. Common reasons include:
Not Medically Necessary": 48% of denials fall into this category.
Undocumented Step Therapy: Accounts for 23% of denials.
Missing Documentation: Makes up 30–35% of denials [14][15].Next, request the complete claim file, as federal law entitles you to this information.
The file should include internal notes from the insurer’s medical director and the clinical policy bulletins they relied on [16][17].
This information will help you identify where the disconnect occurred. If the denial is based on medical necessity, request a peer-to-peer review. These direct discussions between your physician and the insurer’s medical director have a 58–65% success rate in overturning denials [15].
"Prior authorization denials are not final. With proper documentation and appeal strategy, you can overturn the majority of these denials and provide necessary care to your patients."
– AJ Friesl, Founder, Muni Health [15]
Once you’ve clarified the reasons for the denial, you can move forward with a strong appeal.
Prepare a Complete Appeal
The foundation of any appeal is the Letter of Medical Necessity (LMN) [17].
This letter should directly address the denial reason, referencing the payer’s medical policy bulletins and demonstrating how your patient meets their criteria [15][18].
Incorporate objective measures like PHQ-9 or GAD-7 scores and cite clinical guidelines from trusted organizations, such as the American Psychiatric Association or ASAM, to support the severity and necessity of the treatment [1][6][17].
For step therapy denials, include detailed documentation of previous treatments, such as dates, dosages, durations, and outcomes [14][17].
If the payer’s mental health requirements seem more restrictive than those for medical or surgical services, consider invoking the Mental Health Parity and Addiction Equity Act (MHPAEA) in your appeal [1][6]. For urgent cases, request an expedited review to receive a decision within 24–72 hours [15][18].
Always submit your appeal through certified mail with a return receipt or via the payer’s portal, taking a screenshot for confirmation.
Be mindful of deadlines, as most plans allow 60–180 days for first-level appeals [6][16]. By following these steps, you can maximize your chances of overturning denials and ensuring timely care for your patients.
Assign Team Roles and Improve Workflows
Preauthorization issues often stem from inconsistent processes. Physicians already dedicate an average of 16 hours per week to prior authorization tasks [19]. The key isn’t working harder - it’s creating a system where every team member has a clear understanding of their responsibilities. Assigning precise roles enhances preauthorization steps and boosts workflow efficiency.
Define Staff Responsibilities
To ensure smooth preauthorization, assign specific responsibilities for each step of the process. Every task should have a primary owner and a backup to maintain continuity.
Here's how roles can be distributed:
The Scheduler or Intake Coordinator verifies the payer-service matrix during booking and opens the case immediately.
The Utilization Management (UM) Specialist handles assembling clinical packets, starting submission timers, monitoring statuses, and managing renewals - submitting them 14 days before expiration or when 75% of authorized units are used [1].
The Clinical Lead ensures all documentation meets medical necessity criteria, such as LOCUS, CALOCUS, or ASAM, and approves complex requests.
The Billing QA checks claims to ensure they include a valid authorization number, accurate dates, and sufficient units in Box 23 before submission.
The Operations Lead oversees the payer-service matrix, tracks weekly performance metrics, and addresses process issues when metrics fall below acceptable levels [1].By clearly defining these roles, errors are minimized, and accountability is strengthened at every stage.
"Prior authorization is where revenue leaks and treatment stalls, not because payers are impossible, but because processes are inconsistent."
– Lisa Martin, Mental Health Specialist, AnnexMed [1]
Improve Preauthorization Processes
Defined roles are only part of the solution - refining workflows is equally important. Start by creating a payer-service matrix, a dynamic grid that outlines high-volume services, whether preauthorization is required, typical authorization spans, and the necessary documentation for each payer [1].
With clear roles in place, standardize procedures to cut delays. Use SLA timers to trigger alerts at 24-, 48-, and 72-hour intervals [1].
Streamline clinical packets with templates that align with reviewer checklists, incorporating validated assessment scores like PHQ-9 and GAD-7, along with functional impairment documentation [1].
Conduct weekly huddles to review performance dashboards tracking KPIs, such as "no-auth" denial rates (aiming for less than 1%) and average decision times [1].
Pay attention to approval trends by payer; consistently high approval rates may qualify for "gold card" benefits, reducing or waiving preauthorization requirements [1][19].
"The cure is a boring, repeatable machine that runs the same way on a hectic Tuesday as it does on a quiet Friday."
– Lisa Martin, Mental Health Specialist, AnnexMed [1]
Use Opus Behavioral Health EHR for Automation
Switching from manual workflows to automation with Opus Behavioral Health EHR can make preauthorization tasks much smoother.
Manual processes often waste time and increase the risk of errors, but Opus simplifies things by automating everything - from documentation to renewal tracking. With its AI-powered documentation, the platform cuts clinical documentation time by an impressive 40% [21]. This time-saving feature allows staff to focus more on delivering quality patient care.
Automate Documentation and Submission
Opus takes care of the heavy lifting by automatically pulling validated assessment scores, such as PHQ-9 and GAD-7, directly from patient records into authorization packets. This eliminates the need for manual entry, reducing transcription errors [1][22].
The system also uses mandatory fields to ensure all submissions are complete, capturing essential signatures and 42 CFR Part 2 consents before sending [22].
Authorization packets are formatted with standardized templates, including DSM-5-TR diagnoses, LOCUS/ASAM rationale, and measurable treatment goals - exactly what payers require [1]. Additionally, all communications are logged automatically for compliance audits [20].
"This process will simplify our operations to save so much time. We will no longer have to manually pull so many charts per quarter and have a timelier billing process for quicker reimbursements."
– Amanda Wilson, Director of Clinical Services, Mental Health and Substance Use Treatment Center [21]
This automated approach integrates seamlessly with real-time tracking features, ensuring that every step is monitored efficiently.
Track Preauthorization Status
Opus provides a dashboard that tracks critical details like request dates, authorization numbers, and units used - all in real time [1]. Automated alerts notify staff 14 days before an authorization expires or when 75% of authorized units have been used, preventing costly gaps in billing [1].
The platform also includes an outcomes measurement tool that offers instant feedback on patient progress. With access to 140+ detailed reports, staff can identify potential denials before they impact revenue [21]. Automated reminders further improve efficiency, reducing appointment no-shows by up to 75% [20], which helps maintain a consistent treatment history - key for successful renewals.
"We are excited to expand our ability to track and report on data so that we can improve our quality assurance and reporting processes."
– Jennifer Gozy, PsyD, LP, Director of Clinical Systems and Compliance, Care Counseling Clinics [21]
Conclusion
Efficiently managing payer preauthorization starts with building consistent, repeatable processes.
By standardizing tasks like verifying coverage, gathering documentation, submitting requests, and tracking renewals, you remove much of the uncertainty that can lead to claim denials and delays in treatment.
Mental health claims face a denial rate of 15–20%, compared to just 5–10% for medical claims. What's more, 50–65% of these denials are preventable with better processes in place [6][14].
This highlights the importance of refining internal workflows. Each step, from confirming coverage to monitoring renewals, should be standardized to reduce denials and ensure patients get timely care.
Successful practices assign clear responsibilities: one team member focuses on payer guidelines, another prepares clinical packets, and a third keeps track of authorization deadlines. Staying ahead of regulatory changes is equally crucial.
For example, the CMS 2026 rule will require payers to respond to standard preauthorization requests within 7 calendar days [7]. Meeting such deadlines demands either highly efficient manual workflows or automation tools to handle repetitive tasks.
"Prior authorization is where revenue leaks and treatment stalls, not because payers are impossible, but because processes are inconsistent." – Lisa Martin, Mental Health Specialist [1]
To streamline this process even further, automation with tools like Opus Behavioral Health EHR can make a significant difference.
Automated systems can pull clinical scores, format packets to meet payer requirements, and send alerts before authorizations expire. This frees up valuable time, allowing your team to focus on delivering exceptional patient care.
With well-organized workflows and smart technology, you can reduce denials, speed up approvals, and ensure patients stay on track in their recovery journey.
FAQs
What’s the fastest way to know if a CPT code needs prior auth for a specific payer?
To find out if a CPT code needs prior authorization, refer to the payer's official prior authorization list or guidelines, which are typically accessible through their portal or documentation.
Many payers clearly outline which codes or services require prior approval. Additionally, using automated tools or EHR-integrated solutions - such as Opus Behavioral Health EHR - can simplify this process by quickly checking prior authorization requirements.
What should I include in a 'reviewer-ready' mental health prior authorization packet?
A well-prepared mental health prior authorization packet should make it easy for reviewers to assess the case by including clear and up-to-date documentation that supports the need for treatment and meets coverage requirements. Essential elements to include are:
Clinical notes and progress reports: These provide a detailed overview of the patient's condition and treatment history.
Treatment plans and goals: Clearly outline the therapeutic objectives and how they address the patient's needs.
Evidence supporting medical necessity: Include documentation that justifies why the treatment is required.
Test results or assessments: Any diagnostic tools or evaluations that back up the clinical findings.
Related correspondence: Letters or communications that provide additional context or clarification.Arranging these materials in a logical, easy-to-navigate format can help minimize delays, reduce the chance of denials, and streamline the authorization process.
How can I prevent authorization lapses when ongoing therapy needs renewals?
To keep authorization lapses at bay, it's crucial to have a clear and organized renewal process in place. Here’s how you can stay ahead:
Submit Renewal Packets on Time: Ensure all necessary documents are completed and submitted well before deadlines.
Assign Follow-Up Responsibilities: Designate someone to handle follow-ups and monitor the status of renewals.
Track Expiration Dates: Use a system to keep tabs on upcoming expiration dates to avoid last-minute scrambles.Additionally, maintaining open communication with payers and leveraging tools like parity or gold-card rules can help reduce the need for reauthorizations. These practices not only streamline the renewal process but also minimize the risk of treatment delays for patients.
