
Behavioral health EMR systems are vital for managing therapy documentation, tracking patient progress, and ensuring compliance with regulations like HIPAA and 42 CFR Part 2.
But many organizations struggle with implementation, leading to inefficiencies, lost revenue, and compliance risks.
Here are the five biggest mistakes to avoid:
Using Generic Software: Generic EHRs often lack tools like DSM-5 integration, group therapy documentation, and ASAM workflows, making them unsuitable for behavioral health needs.
Skipping Training: Insufficient training can lead to productivity losses, staff burnout, and costly turnover. Structured onboarding and role-specific training are critical.
Poor Data Migration: Errors during migration can result in lost patient data, compliance issues, and financial penalties. A phased and quality-controlled approach is essential.
Ignoring Revenue Cycle Setup: Behavioral health billing is complex. Failing to configure systems for tracking authorizations and payer-specific rules can lead to high denial rates and revenue losses.
Stopping at Go-Live: Go-live is just the beginning. Without ongoing support, staff feedback, and system audits, inefficiencies and dissatisfaction can derail success.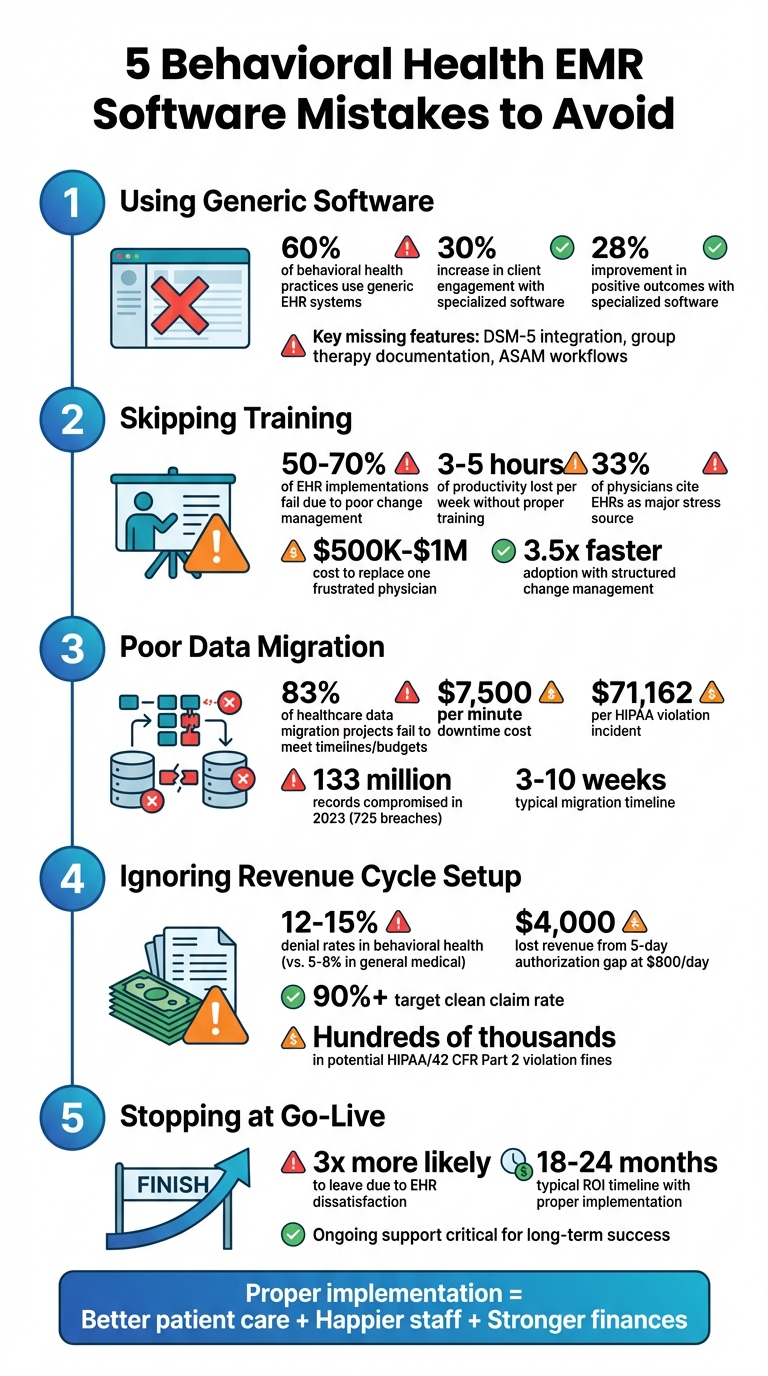
5 Critical Behavioral Health EMR Implementation Mistakes and Their Impact
The biggest MISTAKES therapists make with Electronic Health Records (EHR)
1. Selecting Software That Doesn't Support Behavioral Health Workflows
More than 60% of behavioral health practices use generic EHR systems that aren't designed to meet their specific needs [8].
These systems are built for quick, checkbox-driven visits, which is a stark contrast to the demands of behavioral health.
Here, clinicians often conduct 50-minute therapy sessions, document detailed narratives, track long-term progress, and perform psychosocial assessments [8].
Industry professionals highlight this mismatch clearly:
"Primary care EHRs were built for 15-minute medical visits with checkboxes and vital signs. Behavioral health runs on 50-minute sessions with narrative documentation." - The PIMSY Team [8]
Generic EHRs often fall short in providing essential tools for behavioral health.
They typically lack DSM-5 integration, specialized templates like SOAP or DAP notes, and group therapy features that allow clinicians to document once for multiple patients [8].
For addiction treatment centers, the gaps are even more pronounced, with missing tools such as ASAM multi-dimensional assessment forms, level-of-care recommendation logic, and tracking for medications like buprenorphine or methadone used in MAT (Medication-Assisted Treatment) [7].
This lack of tailored features also creates regulatory challenges. Behavioral health data requires strict compliance with 42 CFR Part 2 in addition to HIPAA.
This includes workflows for consent-based record releases and the segregation of substance use treatment information [7][8]. Without these capabilities, practices risk both non-compliance and diminished care quality.
On the other hand, organizations that adopted specialized behavioral health software saw a 30% increase in client engagement and a 28% improvement in positive outcomes [8].
When evaluating vendors, it's crucial to look for features like group therapy documentation, ASAM workflows, and built-in compliance with 42 CFR Part 2. These tools can make a significant difference in both operations and patient care.
2. Skipping Proper Training and Change Management
Even the most advanced behavioral health EMR can fall flat without adequate staff training.
In fact, 50% to 70% of EHR implementations face major adoption issues - not because of the technology itself, but due to poor change management [9].
When clinicians aren't properly trained, they can lose 3 to 5 hours of productivity each week trying to navigate inefficient workarounds.
This not only disrupts workflows but also contributes to burnout. Over 33% of physicians identify EHRs as a significant source of stress [2][4][9]. The financial consequences are just as alarming: replacing a single physician who leaves due to frustration can cost anywhere from $500,000 to $1 million [9].
The gap in training is clear. Clinicians who receive 11 or more hours of onboarding training report much higher satisfaction compared to those who only get the bare minimum of 3 hours.
Organizations with structured change management plans also hit their adoption targets 3.5 times faster [9]. These numbers highlight how crucial it is to invest in comprehensive training programs.
"Technology is rarely the root cause - change management is."
– EHR Source [9]
It's also important to tailor training to specific roles. A psychiatrist documenting a 50-minute therapy session has vastly different needs than front desk staff handling appointments or billing teams processing claims.
To address this, top-performing organizations designate one clinical champion for every 10–15 users. These champions often receive compensation of $5,000–$15,000 or 10–20% protected time to provide peer support.
Additionally, successful organizations allocate 15–20% of the total project budget to change management. This funding typically covers training materials, temporary staffing, and reduced patient volumes during the critical first 2–4 weeks of go-live [9].
3. Poor Data Migration and Lack of Documentation Standards
Once training and change management are addressed, the next challenge is ensuring data integrity during system migration.
Mistakes in this phase can have serious consequences, particularly for patient safety. Did you know that 83% of healthcare data migration projects fail to meet their original timelines or budgets? [13].
When migration errors occur, critical information - like medication lists, allergy details, or suicide risk assessments - can be lost, directly putting patients at risk [11][12].
The financial stakes are also high. Downtime can cost $7,500 per minute, and HIPAA violations carry fines of up to $71,162 per incident [13]. In 2023 alone, over 133 million records were compromised across 725 healthcare data breaches, many of which were linked to system transitions [13].
"Without proper checks, critical information like medication history or diagnoses can be lost during migration. Always back up your existing data and thoroughly test a sample dataset after migration."
– Sanjiv Patel, VP of Product, ICANotes [12]
A phased migration strategy is one way to reduce these risks. Start small by migrating 5–10% of your data in a pilot phase.
This helps uncover mapping errors before moving forward with the full transition [11]. Before migration begins, standardize your documentation by cleaning up records, removing duplicates, consolidating terminology (like DSM-5 and ICD-10), and archiving outdated files.
Collaborate with clinical teams to map fields from the legacy system to the new platform, ensuring that unstructured data - such as therapy notes or scanned documents - transfers correctly [11][12].
Throughout the migration process, enforce strict quality controls. For example, keep both the old and new systems accessible for 2–4 weeks after the go-live date.
This allows teams to log notes in both systems and quickly catch any discrepancies [13].
After the migration, conduct audits by cross-checking migrated records against the originals, focusing on high-risk data. When done right, behavioral health data migration typically takes 3 to 10 weeks [12].
Rushing this process not only compromises patient safety but also leads to more cleanup work later. Taking a careful, methodical approach ensures the foundation for smooth revenue cycle management.
4. Overlooking Revenue Cycle and Reporting Setup
Once data migration is complete, setting up a solid revenue cycle is a must to keep your cash flow steady.
Skipping this step can lead to serious revenue disruptions. For example, denial rates in behavioral health typically range from 12% to 15%, which is about double the 5% to 8% seen in general medical practices [14].
Many of these denials happen because of configuration issues that weren’t addressed during the initial setup. These gaps don’t just hurt cash flow - they can also create compliance headaches.
"Authorization management is the single most impactful revenue cycle function in behavioral health."
– ehrsource.com [14]
Behavioral health billing has unique requirements that general medical billing doesn’t cover. For instance, a 5-day authorization gap at $800 per day can mean $4,000 in lost revenue [14].
To avoid this, your EMR should be set up to track authorized units and send alerts when usage hits 80% or when only 5 days remain before expiration [14].
It also needs to log exact start and stop times for psychotherapy codes since even small timing discrepancies can lead to claim rejections [14][16].
Strong reporting tools are just as important for staying compliant. If your system doesn’t offer real-time alerts or automated audit trails, you’re at higher risk during Medicaid or payer audits [5][3].
HIPAA or 42 CFR Part 2 violations can result in fines reaching hundreds of thousands of dollars [5]. Without detailed reports on clean claim rates, accounts receivable timelines, or denial reasons, it’s nearly impossible for leadership to accurately forecast revenue or pinpoint financial leaks [5][16].
Addressing these revenue cycle details ensures your clinical and financial systems work together smoothly.
To optimize billing, implement hard stops that prevent note signing if critical timing or consent details are missing [14][15].
Use claim scrubbing to check for payer-specific rules, such as modifiers like -95 for telehealth or -HO for master's level providers, before submission [15][16].
Your clean claim rate should stay above 90%. If it drops below that threshold, audit for recurring issues like missing modifiers or incorrect NPIs [15].
"Small process gaps multiply fast when you're billing hundreds of recurring therapy sessions per month."
– Supanote [15]
5. Treating Go-Live as the Final Step
After perfecting your revenue cycle and reporting setup, it’s important to recognize that the journey with your EMR doesn’t stop at go-live - it’s just getting started.
Many organizations celebrate go-live as if the hard work is behind them. In reality, it’s only the first chapter. The early weeks of live operation often expose workflow inefficiencies, clunky templates, and unexpected technical hiccups. Without a solid post-go-live plan, these issues can frustrate staff and derail system adoption.
"Go-live is just the beginning. What the implementation team learns during that first week should directly influence how they support the practice over the following months."
– ProsperityEHR [10]
Post-go-live support is as critical to success as data migration and revenue management. Dissatisfaction with an EHR can have serious consequences - studies show that unhappy staff are three times more likely to leave their roles [6].
To prevent this, designate a post-go-live lead to act as the main point of contact with your vendor.
This person can coordinate follow-up training sessions to dive into advanced features that may have been overlooked during initial onboarding. Keep a close eye on metrics like documentation time, clean claims rates, and system uptime to identify and tackle issues early.
Regular staff feedback is invaluable. Use surveys and forums to gather insights, as clinicians often create workarounds when workflows or templates don’t align with their needs.
These workarounds are a red flag that your configurations may need adjustments. Additionally, reviewing audit logs and role-based access permissions is essential to maintaining compliance with HIPAA and 42 CFR Part 2.
Think of your vendor as a long-term partner.
As your organization grows and regulations evolve, your EMR must adapt too. Regular system audits and performance reviews will help ensure your technology evolves to support both clinical and financial goals. By prioritizing these post-go-live efforts, you’ll ensure your EMR grows alongside your practice’s needs and continues to deliver value.
Conclusion
Implementing a behavioral health EMR is about more than just adopting new technology - it’s about laying the groundwork for improved patient care, happier staff, and stronger financial health.
The five mistakes highlighted here - selecting software that doesn’t align with behavioral health needs, neglecting thorough training and change management, rushing data migration without proper standards, overlooking revenue cycle setup, and viewing go-live as the endpoint - are common missteps that can derail even the best intentions.
These errors can ripple through your practice, affecting clinical efficiency, compliance, and financial performance.
Poor implementation often leads to increased clinician burnout and costly staff turnover, while ignoring revenue cycle setup can result in steep revenue losses and hefty compliance penalties, sometimes reaching into six figures [4][6][1][2].
The upside?
Practices that follow proven implementation strategies often see a full return on their EMR investment within 18 to 24 months [2].
The key is to treat your EMR as a long-term partner.
Establish a governance committee to oversee ongoing improvements, perform regular system audits to address workflow challenges, and maintain a super-user program to support staff as processes evolve.
Don’t forget to allocate funds for yearly updates and refresher training - these aren’t just expenses; they’re investments in your practice’s future.
When compliance, efficiency, and patient outcomes work in harmony, the benefits are undeniable. Features like built-in 42 CFR Part 2 safeguards and automated audit trails not only protect your practice legally but also streamline daily operations.
Tools for measurement-based care provide actionable insights that enhance treatment outcomes, while a well-structured revenue cycle ensures fair compensation for the specialized care you deliver. Together, these elements create a solid foundation for growth.
Your EMR should grow with your practice, adapting to new regulations, payer demands, and advances in care.
By steering clear of these common pitfalls and committing to ongoing system refinement, you position your practice for long-term success. Every improvement you make strengthens your practice against operational and financial challenges.
FAQs
How do I know if an EMR truly fits behavioral health workflows?
To find an EMR that aligns with behavioral health workflows, focus on features tailored to your needs. Look for customizable documentation templates, specialized billing tools, and compliance support.
Steer clear of systems designed for general or multi-specialty use, as they often miss the nuances required for behavioral health practices.
Take advantage of demos or trials to explore the system’s functionality. Involve your team in the evaluation process to ensure it meets your unique requirements, like treatment planning and outcome tracking.
This collaborative approach helps confirm the EMR supports the specific processes essential to your practice.
What should a training plan include before and after go-live?
A solid training plan for an EMR system involves two key stages: preparing staff before go-live and providing ongoing support afterward.
Before the system goes live, it's crucial to ensure that staff are well-trained on workflows, documentation requirements, and compliance protocols.
This phase should also include establishing a dedicated support team to handle any troubleshooting needs that may arise during the transition.
Once the system is live, the focus shifts to maintaining momentum. Offer continuous support to address any issues, conduct refresher training sessions to reinforce key skills, and schedule regular feedback meetings.
These steps help tackle challenges as they come up and fine-tune processes to improve overall efficiency.
By prioritizing both preparation and ongoing support, you can boost staff confidence and make the most of the EMR system's potential.
What data should we validate first when migrating to a new EMR?
When migrating to a new EMR system, the first priority is to validate the accuracy and completeness of your current patient information.
This includes carefully reviewing provider notes, organizational metrics, billing records, and protected health information (PHI). Ensuring this data is both accurate and properly formatted is essential to avoid disruptions and ensure compliance during the migration process.
- Behavioral Health
- EHR Systems
- Addiction Treatment EHR
- Telehealth
- mental health
- addiction treatment
- Behavioral health facility
- behavioral Health center
- HIPPA Compliant
- PTSD
- ehrsoftware
- Depression
- Substance Abuse Disorder
- Anxiety
- MentalHealthMatters
- RCM
- claim denials
- clinical documentation
- hipaa
- mental health awareness
- screening tools

July 28, 2026

July 27, 2026

July 24, 2026

July 23, 2026

July 22, 2026

July 22, 2026
Recommended Posts
.png)
Wednesday, November 05, 2025
Reduce Documentation Time: 6 Proven Strategies
Clinicians in behavioral health often face overwhelming documentation demands, which can lead to stress, errors, and ...

Friday, February 11, 2022
Top Considerations for Behavioral Health Treatment Centers When Switching EHR Systems
The world is cautiously beginning to open again after the Covid-19 shelter-in-place orders are lifted. While it’s ...

Tuesday, December 09, 2025
AI-Powered EHR Tools for Behavioral Health
AI-powered EHR tools are transforming behavioral health practices. These tools reduce paperwork, improve documentation ...