Payer contracts directly impact your revenue.
But many behavioral health organizations neglect regular reviews, leading to claim denials and underpayments.
Here's what you need to know:
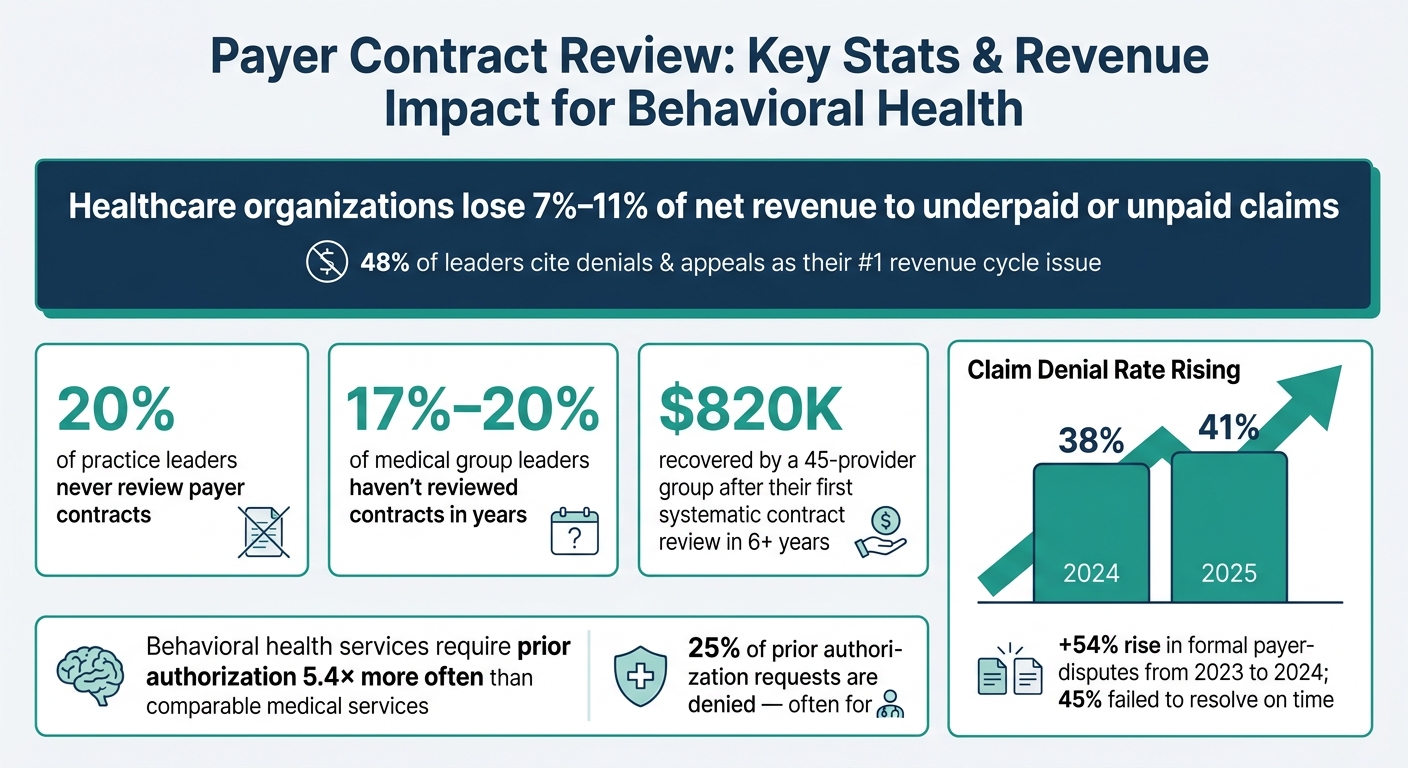
20% of practice leaders don’t review contracts, risking missed revenue.
Claim denial rates rose from 38% in 2024 to 41% in 2025, with organizations losing 7%-11% of net revenue due to underpaid or unpaid claims.
Common pitfalls include outdated reimbursement rates, short filing deadlines, and vague contract terms allowing unilateral changes.
Behavioral health services face higher denial risks, with 25% of prior authorization requests denied.
Key Takeaways:
Reimbursement Rates: Compare top CPT codes to ensure payers meet contracted rates. Behavioral health rates typically range between 110%-180% of Medicare.
Authorization Rules: Stay ahead of prior authorization requirements, especially for high-risk services like IOP and residential care.
Timely Filing: Map out deadlines (usually 30-180 days) and integrate them into workflows to avoid denials.
Centralize Contracts: Organize agreements in a digital repository, focusing on high-revenue payers.
Use Technology: Automate contract management to catch underpayments and streamline compliance.Regular reviews, data-driven analysis, and integrating contract terms into daily operations can prevent revenue losses and reduce administrative burdens.
Payer Contract Review: Key Stats & Revenue Impact for Behavioral Health
Key Elements of Payer Contracts to Review
When reviewing payer contracts, it’s crucial to focus on the sections that influence payment decisions the most. Prioritizing these areas can save time and help safeguard your revenue.
Reimbursement Rates and Fee Schedules
Start by examining fee schedules at the level of individual CPT or HCPCS codes. Why? Because payers sometimes input incorrect rates after contracts are finalized. Without a detailed code-level review, these errors can remain unnoticed for months, potentially costing your practice thousands.
The Medicare Physician Fee Schedule (MPFS) serves as the standard benchmark for reimbursement rates.
Commercial rates for behavioral health services typically range between 110% and 180% of Medicare, influenced by factors like specialty and market conditions. If your rates fall below this range, you might be losing out on significant revenue opportunities.
A good strategy is to focus on your top 25 CPT codes by revenue and cross-check them against your contracted rates. For time-based codes (e.g., 90832, 90834, 90837), ensure that the documentation aligns with the billed durations. Discrepancies in this area are a common reason for recoupments during audits.
"Cigna didn't even know that its rates were below Medicare. But I was the only one who called." - Lynne Leis, Practice Administrator, Physicians Practice [2]
Pay attention to behavioral health carve-outs, too. Many commercial plans delegate mental health and substance use disorder claims to Managed Behavioral Health Organizations (MBHOs) like Optum, Carelon, or Magellan.
If claims are mistakenly sent to the medical payer instead of the MBHO, they may be denied - not because the service isn’t covered, but because it was submitted to the wrong entity.
Once you’ve reviewed reimbursement rates, shift your attention to authorization and utilization management requirements.
Authorization and Utilization Management Requirements
Terms around service authorization carry just as much weight as reimbursement rates. Prior authorization is a significant driver of denials in behavioral health billing.
In fact, behavioral health services require prior authorization 5.4 times more often than comparable medical services [8], with around 25% of initial requests denied, often for reasons like "insufficient information" [5].
Contracts specify the clinical criteria payers use to assess medical necessity. For substance use disorder (SUD) services, this typically involves meeting ASAM Criteria.
For mental health services, payers may rely on tools like LOCUS, InterQual, or their proprietary guidelines. Understanding which framework is used allows your clinical team to document services in a way that aligns with payer expectations.
Utilization management (UM) intervals are another critical consideration. For residential care, concurrent reviews might occur every 7 to 14 days. For PHP (Partial Hospitalization Program) and IOP (Intensive Outpatient Program) services, about 80% of commercial plans require prior authorization [6].
Re-authorization requests should be submitted when only 2 to 3 sessions remain - waiting until the current authorization expires can lead to automatic denials with no option for appeal.
"Missing, expired, or wrong-level authorizations represent one of the most preventable causes of behavioral health claim denials." - Cipher Billing [7]
Timely Filing and Appeals Deadlines
Timely filing and appeals deadlines are non-negotiable when it comes to preserving reimbursement. Missing these deadlines often results in irreversible denials.
Filing windows generally range from 30 to 180 days after the date of service, depending on the payer. Appeals deadlines vary as well, with some payers allowing up to 180 days to contest a denial, while others provide as little as 30 days.
These terms are negotiable, so shorter windows should be addressed during contract negotiations.
"A one-day delay in portal submissions can trigger both clinical and financial exceptions." - Behave Health [4]
When reviewing contracts, create a clear map of all filing and appeals deadlines for your highest-volume payers. Integrate these dates into your billing workflows to ensure timely submissions.
Managing deadlines proactively is far more effective than dealing with reactive appeals. In 2024, formal payer-provider disputes rose by 54% compared to 2023, with 45% of disputes failing to reach a resolution in time [1].
Staying ahead of these deadlines is one of the simplest ways to avoid unnecessary revenue loss.
Building a Structured Contract Review Process
Establishing a structured process for contract review is essential to safeguard revenue and ensure consistent performance over time.
Creating a Centralized Contract Repository
Gather all contracts into a single, digital repository to streamline monitoring and management. This repository should include base agreements, fee schedules, amendments, and policy bulletins.
Prioritize contracts by their revenue impact - data shows the top three payers often account for 50% to 70% of total collections [9]. These high-impact contracts deserve the most attention.
Key details to extract include allowable rates by CPT code, modifier rules, timely filing deadlines, and prior authorization requirements. Set up alerts for auto-renewal deadlines, as most contracts require notice 90 to 120 days before expiration [9].
Additionally, flag contracts that haven’t been reviewed in over two years - studies indicate that 17% to 20% of medical group leaders fail to review payer contracts regularly [9].
The repository should also highlight carve-out arrangements, where organizations like Optum or Magellan manage behavioral health benefits independently from the main medical plan [4].
"Until every agreement is centralized, you cannot evaluate the portfolio." - PayerPrice [9]
Once centralized, this repository becomes a powerful tool for analyzing payer performance and identifying revenue gaps.
Analyzing Payer Mix and Denial Data
With contracts organized, focus on evaluating each payer’s performance by diving into the data at the CPT code level.
One often-overlooked issue is silent underpayments- claims that appear resolved but are paid below the contracted rates.
For example, if a commercial payer reimburses 5% less than the agreed rate on a frequently billed code, this discrepancy may not appear on standard dashboards unless actively monitored [3].
A multispecialty clinic, for instance, recovered $250,000 in underpayments over 18 months by systematically comparing payments to contracted fee schedules [9].
Volume-weighted analysis is also critical when assessing proposed rate increases. A 3% increase might sound beneficial, but if it applies only to low-volume codes, it could have little to no impact on overall revenue.
"If you take the word that it's a 3 percent increase, it might not be to revenue. Simply because of where the increases are happening on the fee schedule." - Mark Schroeder, VP of Growth, Aroris Healthcare [9]
To gauge the real impact, multiply each CPT code’s proposed rate change by its 12-month billing volume. Also, track payer-specific metrics like denial rates, prior authorization approval rates, and days to payment. These figures help quantify the administrative burden of each payer, a key consideration during contract renegotiations.
This data-driven approach lays the groundwork for leveraging technology to optimize contract management.
Using Technology for Contract Management
Relying on manual processes for contract management is inefficient and prone to errors. While manual reviews handle 8–12 claims per hour, automated systems can process hundreds, checking against over 80,000 payer-specific rules simultaneously [3].
Spot-checking in manual workflows often leads to missed issues, such as underpayments.
The best solution is to adopt technology that integrates seamlessly with existing EHR systems, avoiding the need for separate data migrations. For instance, platforms like Opus Behavioral Health EHR combine revenue cycle management with advanced reporting tools directly within the clinical workflow.
This setup allows billing teams to access denial data and payer performance metrics without disruption. With more than 140 reporting options, Opus enables CPT-level analysis to catch underpayments and monitor payer trends over time.
"The most effective contract analysis happens before the claim leaves the building. Prevention scales. Recovery does not." - Exactrx [3]
Best Practices for Detailed Contract Reviews
When it comes to maximizing revenue, the real battleground isn't in billing - it’s in the fine print of your contracts. A meticulous, line-by-line review of every agreement is essential. This step ensures you're not leaving money on the table or exposing your practice to unnecessary risks.
Identifying High-Risk Contract Terms
Some clauses in contracts can pose significant risks to your revenue. For instance, unilateral amendment clauses let payers change reimbursement rates or coverage policies mid-contract without your approval.
Similarly, vague medical necessity language that grants payers "sole discretion" to define coverage criteria can lead to unpredictable denials.
Another red flag is retrospective audit rights, which allow payers to review and recoup payments on claims that were already processed. To protect your revenue, negotiate a lookback period that’s capped at 12 months or aligns with your state’s statutory maximum, whichever is shorter [2].
As Garvit Chouhan, Head of RCM Delivery at Neolytix, explains:
"Payer contracting is not an administrative formality. It is one of the most consequential decisions a practice makes, and one that compounds over time either in its favor or against it." [1]
Verifying Appeal and Dispute Processes
Every contract should outline a clear and actionable process for challenging denials and recovering underpayments. If this process is unclear or absent, you’re essentially operating without a safety net.
Key points to negotiate include requiring that clinical appeals be reviewed by a same-specialty clinician and ensuring that downcoding only occurs after a thorough review of documented medical records, with written justification provided [2].
The need for clear dispute resolution processes is becoming increasingly urgent. In 2024, there were 133 formal payer-provider disputes - a 54% jump from 2023 - and nearly 45% of these cases failed to reach a timely resolution [1]. Without explicit dispute language in your contracts, your practice could face prolonged and costly revenue interruptions.
Additionally, contracts must reflect current payer policies to avoid silent denials, which can occur when policies change without formal notice.
Aligning Contracts with Payer Policies
A common mistake in contract management is assuming that the signed agreement is the full story. Many payer contracts reference external documents - like policy manuals, clinical guidelines, and fee schedules - which hold the same legal weight as the contract itself.
These documents can be updated unilaterally by payers, often without formal amendment notices, leading to unexpected denials [1].
Athena Doshi highlights the importance of proactive monitoring:
"Payer policy changes happen quietly. Fee schedules shift without fanfare. A commercial payer reimbursing 5% below the contracted allowable on a high-volume CPT code will not show up on any dashboard unless something is actively watching for it." [3]
To stay ahead, ensure your billing and coding teams have access to the latest versions of payer manuals and fee schedules.
Regularly cross-reference contract terms with current payer policies. Catching discrepancies before claims are submitted is far more efficient than dealing with denials after the fact [3].
Integrating Contract Terms into Daily Operations
After reviewing contracts, the next step is to weave their terms into daily operations. This ensures your revenue remains protected. It's not enough to simply review a contract; its terms must actively guide everyday processes - whether that's billing, front desk procedures, or clinical documentation. Without this practical application, even the most carefully crafted contracts can fall short of their purpose.
Turning Contract Terms into Workflow Steps
Create payer-specific checklists that turn contract terms into clear, actionable steps for your team.
For instance, if a payer requires prior authorization for residential care within 24 hours of admission, this requirement should be a defined step in your intake process - not buried in dense contract language.
Identify the riskiest contract terms and align them with critical workflows, such as eligibility verification, clinical documentation, and claim submissions. Encourage your team to prioritize claims based on each payer’s filing deadlines to reduce the risk of denials [2].
To simplify access to essential contract details, develop a one-page summary that highlights key points like renewal dates, amendment windows, filing deadlines, and high-risk clauses. This approach saves time and keeps vital information at your staff’s fingertips [2].
These streamlined processes pave the way for system automation.
Configuring Systems to Meet Contract Requirements
Ensure your systems are configured to reflect contract terms accurately. For example, load contracted fee schedules at the CPT code level so that your system can automatically compare payments against agreed-upon rates.
Matt Basham, Associate Management Consultant at DoctorsManagement, explains:
"Very few systems, and even fewer billing workflows, include a step where the posted payment is compared against the amount the payer was contractually obligated to pay." [9]
This system-based approach can help detect "silent underpayments", where claims show a zero balance despite the payer remitting less than the contracted amount.
One multispecialty clinic recovered $250,000 in underpayments over 18 months by implementing a system to flag these discrepancies [9].
For behavioral health organizations using platforms like Opus Behavioral Health EHR, integrated RCM tools can automate payer-specific billing rules, send renewal alerts, and monitor denial trends. These features ensure that contract compliance becomes an automatic part of daily operations.
Training Staff on Payer Requirements
Even the most advanced systems are only as effective as the people using them. Training your staff on payer-specific contract terms is essential.
Schedule quarterly reviews to assess performance: use Q1 to benchmark, Q2 to identify gaps, Q3 to prepare for renegotiations, and Q4 to audit new rates [2]. After any contract update, conduct a 90-day audit to confirm that new rates have been implemented correctly [2].
Make sure your team understands the difference between credentialing and contracting. Credentialing verifies clinician qualifications, while contracting outlines payment terms. Confusing these two processes can lead to claims being submitted without a valid payment agreement in place [1].
Conclusion
Payer contracts play a critical role in determining your revenue, yet 17% of medical group leaders admit they haven’t reviewed their contracts in years - sometimes as long as five or six years. This oversight can be costly.
Healthcare organizations often lose between 7% and 11% of net revenue due to underpaid or unpaid claims, with 48% of leaders identifying denials and appeals as their biggest revenue cycle issue [9].
To avoid these losses, centralize your contracts, rank them by their revenue impact, and make it a habit to review them every quarter. Use Transparency in Coverage (TiC) data to benchmark rates, validate payments down to the CPT code level, and catch silent underpayments before they snowball.
For example, a 45-provider group practice documented by Medwave recovered $820,000 in additional annual revenue after conducting its first systematic contract review and renegotiation in over six years [9].
Technology can bridge the gap between what’s outlined in your contracts and what happens in your billing workflow. As Exactrx explains:
"The most effective contract analysis happens before the claim leaves the building. Prevention scales. Recovery does not." [3]
For behavioral health organizations, tools like Opus Behavioral Health EHR can automate payer-specific billing rules, monitor denial trends, and send timely renewal alerts. By integrating such platforms, you can transform contract compliance from a labor-intensive task into an automated, seamless process.
FAQs
How often should we review payer contracts?
Payer contracts need to be reviewed at least once a year. Some practices take it a step further by performing quarterly or even monthly audits.
These frequent checks help ensure that the terms of the contracts stay accurate and beneficial. Regular reviews like these can reduce claim denials and lead to better reimbursement rates.
What’s the fastest way to find underpayments by CPT code?
The fastest way to spot underpayments tied to CPT codes is by generating a remittance variance report.
This report compares the payments you’ve received against the expected contract rates, making it easier to identify recurring underpayment trends across specific CPT codes. By zeroing in on these systematic discrepancies, you can speed up your review process and address issues more efficiently.
Which contract clauses are most likely to cause denials?
Clauses that frequently result in denials include ambiguous language around claims processing and documentation, unclear definitions of what constitutes medical necessity, rigid prior authorization requirements, policies allowing unilateral amendments, and short windows for timely filing. These issues can lead to claim rejections or delays, ultimately impacting reimbursement.
