An EHR switch is a money call before it is a software call. If I were sizing up a change, I’d focus on seven numbers: staff hours, note time, denials, days in A/R, net collections, no-shows, and revenue per visit.
Here’s the short version:
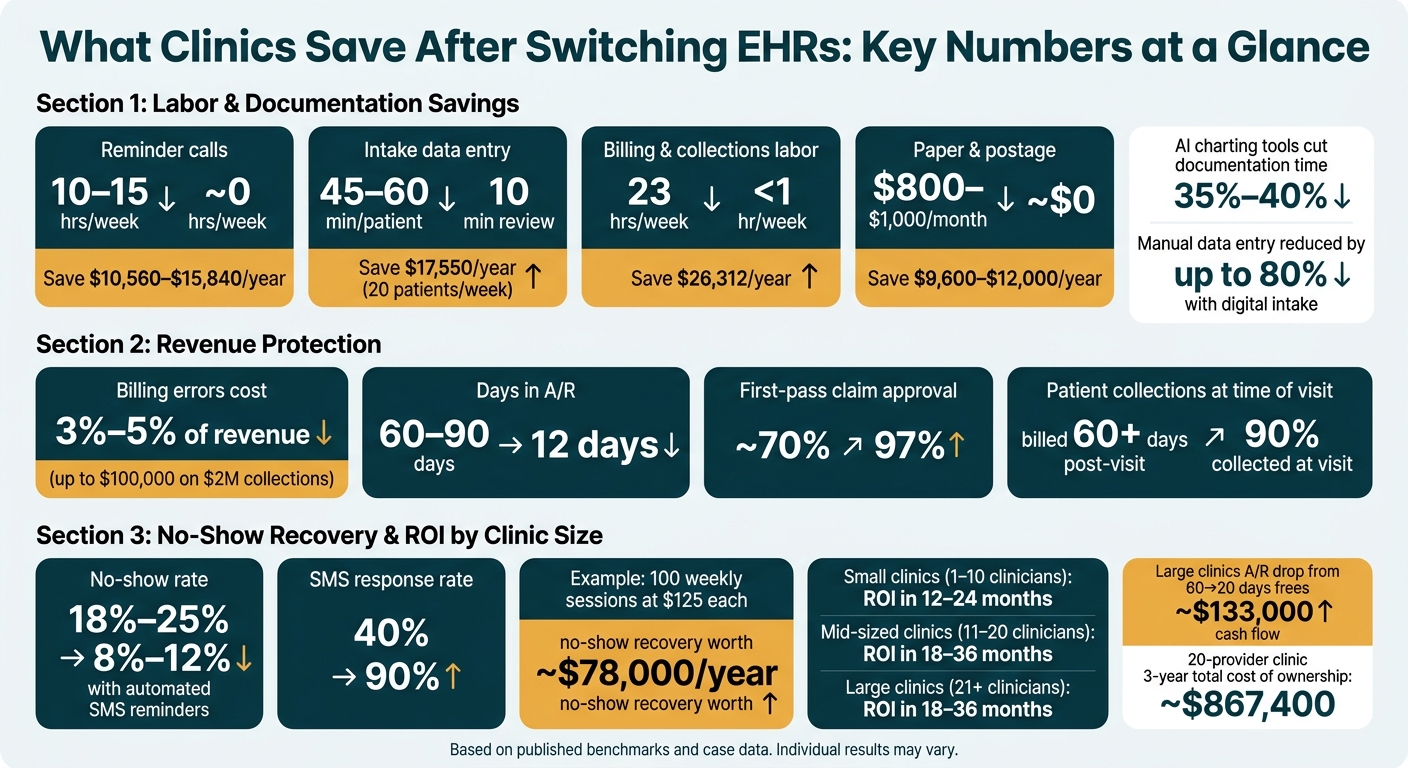
Clinics can cut 10+ hours a week from reminder calls with automation.
Digital intake can trim manual entry by up to 80%.
AI note tools can cut charting time by 35% to 40%.
Billing mistakes can cost 3% to 5% of revenue.
No-show rates can drop from 18%–25% to 8%–12% with automated reminders.
A/R can shrink from 60–90 days to about 12 days in the right setup.
A 20-provider clinic may face about $867,400 in 3-year ownership costs, so tracking payback is not optional.What matters most is simple: Did the switch save labor, protect revenue, and bring cash in faster? If I don’t have a before-and-after scorecard, I can’t answer that.
A few points stand out from the data:
Labor savings show up first. Front desk, intake, billing, and charting are often the first places where hours drop.
Revenue leaks matter fast. Lower denials, fewer billing errors, and shorter note-to-claim lag can mean more cash collected.
Missed visits are expensive. Even a small drop in no-shows can mean tens of thousands of dollars a year.
Clinic size changes the math. Small clinics may feel labor savings first, while larger groups may feel cash-flow relief first.
If I were reading this to judge ROI, I’d use it as a plain scorecard for what to measure before go-live and what to check at 30, 90, and 180 days after launch.
EHR Switch ROI: Key Metrics Before vs. After for Behavioral Health Clinics
Where Clinics Save First: Labor and Documentation Time
Labor savings tend to show up early. Once an EHR is live, clinics can cut repetitive tasks and get hours back across the front desk, billing, and clinical teams.
Workflow Changes That Cut Staff Hours
In a manual setup, the same tasks eat up time day after day: reminder calls, paper intake, printing statements, mailing bills, and general front-desk follow-up.
Reminder calls are a big one. Front desk staff spend 2–3 hours a day on manual reminder calls, and automation can recover 10+ hours a week while pushing response rates from 40% to 90% [3].
Intake paperwork is another major drain. Manual data entry for paper-based intake takes about 45–60 minutes per patient [1]. With digital intake, one staff member can handle 3–4 patients at the same time [1], and manual data entry drops by up to 80% [1].
At $25/hour, that adds up to about $17,550 a year in labor savings for a facility processing 20 admissions per week [1].
Billing outreach adds even more drag. Billing teams can send hundreds of secure payment links in under five minutes, replacing a manual process that usually takes 2–3 days [5]. Just replacing paper billing, including postage and labor, can save $26,000 or more per year [5].
Documentation Time Saved Per Clinician
Clinicians deal with a heavy documentation load too. Modern EHR systems with AI-powered documentation assistants cut charting time by 35% to 40% [7]. In plain terms, that can mean more billable sessions or less charting after hours.
Telehealth friction also costs time. A team of 15 therapists can lose up to 60 hours of billable capacity per week because of login and connection issues in app-based telehealth systems [6]. Browser-based telehealth with a one-tap join can bring that loss close to zero [6].
Labor Savings Before vs. After Go-Live
The table below shows how common workflows shift after go-live:
|
Metric |
Before |
After |
Annual Impact |
|---|---|---|---|
|
Reminder calls (staff hours/week) |
10–15 hours/week [3] |
~0 hours [3] |
$10,560–$15,840 saved (at $22/hr) [3] |
|
Intake data entry (20 patients/week) |
45–60 minutes per patient [1] |
10 minutes of review [1] |
$17,550 saved (at $25/hr) [1] |
|
Billing and collections labor (hours/week) |
23 hours/week [5] |
<1 hour/week [5] |
$26,312 saved (at $22/hr) [5] |
|
Paper and postage costs |
$800–$1,000/month [4] |
~$0 [4] |
$9,600–$12,000 saved [4] |
After labor, the next place clinics tend to see gains is revenue protection: fewer denials, less rework, and faster collections.
Revenue Protection: Fewer Billing Errors, Lower Denials, Faster Collections
After an EHR switch, integrated billing workflows can help protect revenue from the very first claim. That matters because billing mistakes chip away at what a practice should collect. Providers lose an estimated 3%–5% of potential revenue to billing and coding errors. On $2 million in annual collections, that puts as much as $100,000 at risk [8].
How Integrated Billing Workflows Cut Denial-Related Rework
A lot of denials begin long before a claim is sent. The root issue is often a missed eligibility check, incomplete documentation, or a coding gap during the visit itself. Integrated workflows push those checks earlier, when staff can still fix the problem without a scramble later.
For example, clinical templates can require billing-related fields before a note is signed. Charge review edits can flag frequency limits or missing documentation before submission.
And automated prompts can help teams catch missing Advance Beneficiary Notices (ABNs) for Medicare patients before the claim goes out [9][10].
That upstream cleanup can make a big difference. Televero Behavioral Health reported a 97% first-time claim approval rate after moving to an integrated platform [9].
The Dollar Impact of Lower Denial Rates and Fewer A/R Days
The money side is pretty simple: fewer claim issues usually means payment comes in sooner. Televero cut days in A/R to 12 and reached cash-positive status six months early [9]. That's not just a back-office win. It changes cash flow in a way practices can feel.
Integrated systems can also move patient collections closer to the visit. Instead of sending a bill 60+ days after the encounter and hoping it gets paid, proactive workflows let practices collect 90% of patient responsibility at the visit [9].
Denial Rate, A/R, and Collections: Before vs. After
These gains show up in claim approvals, A/R, and what gets collected at the visit.
|
Metric |
Manual/Fragmented System |
Integrated EHR/RCM System |
|---|---|---|
|
Days in A/R |
60–90 days [9] |
12 days [9] |
|
First-pass claim approval |
~70% [9] |
97% [9] |
|
Collections at the visit |
Billed 60+ days post-visit [9] |
90% collected at time of service [9] |
|
Note-to-claim lag |
Manual and delayed |
Automated note-to-claim handoff [10] |
|
Denial-related rework |
Ongoing, staff-intensive |
Reduced through upstream verification and billing edits [9][10] |
Case Study Models: No-Shows, Revenue Capture, and Total ROI
How Lower No-Show Rates Add Up to Recovered Annual Revenue
Once billing workflows get tighter, the next place clinics usually see gains is simple: more visits happen, and more of those visits get paid.
Missed appointments are one of the clearest ways behavioral health clinics lose money. Before automation, clinics often deal with no-show rates between 18% and 25%. After moving to automated SMS reminders, that range often falls to 8%–12% [3].
One mid-sized IOP facility in Texas shows what that looks like in dollars. The clinic ran 100 weekly sessions at $125 per session. At a 22% no-show rate, it was losing $2,750 per week, or about $143,000 per year.
After automated reminders went live, the no-show rate dropped to 10%. That cut weekly losses to $1,250 and recovered almost $78,000 a year [3]. SMS confirmations also pushed response rates from 40% to 90% [3].
That math matters because recovered sessions don't sit in some abstract ROI bucket. They turn straight into annual revenue. And when waitlist alerts refill canceled slots within minutes, clinics protect billable capacity instead of letting it slip away.
Those recovered visits end up carrying a big share of total ROI.
ROI Ranges for Small, Mid-Sized, and Large Clinics
ROI changes by clinic size, but the main drivers stay pretty much the same: labor, denials, collections, and recovered visits.
Small clinics often get to payback first because labor savings and billing automation hit fixed overhead fast. Add faster collections, and many small practices reach measurable ROI within 12–24 months [2].
Mid-sized clinics, with 11–20 clinicians, tend to feel the gains across more parts of the operation. One example is telehealth support time. If clinicians lose 10 to 15 minutes per session to tech issues, a 20-provider clinic can give up about $2,000 per week in lost productivity [6]. Browser-based telehealth and tighter workflows can remove a lot of that drag.
Large clinics, with 21+ clinicians, often feel the biggest impact through cash flow. If A/R drops from 60 days to 20 days on a $200,000 open patient balance, that can free up about $133,000 in near-term cash flow [11].
|
Clinic Size |
Main Savings Drivers |
Typical ROI Timeline |
|---|---|---|
|
Small (1–10 clinicians) |
12–24 months [2] |
|
|
Mid-sized (11–20 clinicians) |
18–36 months [2] |
|
|
Large (21+ clinicians) |
18–36 months [2] |
Labor savings reflect reduced manual reminder calls and documentation time, while revenue uplift comes from recovered no-show visits and faster A/R collections. Figures are based on published benchmarks and case data.
Total Cost of Ownership vs. Annual Net Benefit
The next step is to line up total cost of ownership against annual net benefit and payback timing.
For a 20-provider clinic, 3-year total cost of ownership usually comes in around $867,400, including licensing, implementation, migration, training, hardware, integrations, and maintenance [12]. From there, the core question is pretty direct: do labor savings, lower denials, faster collections, and recovered visits beat annual ownership costs?
The real test happens in the first 6 to 12 months after go-live, when clinics start to see whether those gains show up on the books.
Conclusion: Metrics to Track Before and After Switching
Labor savings, revenue protection, and recovered visits only matter if the clinic tracks them before and after go-live. An EHR switch pays off only when a clinic measures labor, revenue, and no-show changes against a clear pre-switch baseline.
The Baseline Scorecard to Build Before a Transition
Use the same metrics from the ROI sections to judge the switch. Before the move, decision-makers should record seven baseline metrics: admin hours per week, average note completion time, claim denial rate, days in A/R, net collection rate, no-show rate, and average revenue per visit.
That scorecard should also include current intake time, reminder-call hours, billing follow-up time, denial rate, A/R days, collection rate, no-show rate, and revenue per visit. In plain terms, you want a clean “before” picture. Current denial rate and A/R days should serve as part of that pre-switch baseline.
FAQs
How soon can a clinic see ROI after switching EHRs?
A clinic may see ROI in the first month after switching EHRs, mostly from fewer no-shows and less staff time spent on routine work.
Some gains can show up within days or weeks.
Which metrics should we track before go-live?
Before go-live, track a few key operational and financial metrics, including:
Claim acceptance ratesDays in accounts receivable (AR)
Denial patterns
Payment reconciliation
That gives you a clear baseline, so once the switch happens, you can see what changed, what stayed steady, and where problems show up first.
What savings matter most for smaller clinics?
For smaller clinics, the biggest savings usually come from spending less staff time on manual reminders and admin work, cutting no-show rates by up to 30%, and reducing paper billing costs.
Taken together, these changes can improve revenue and make day-to-day work run more smoothly.
