Behavioral health organizations handle some of the most sensitive healthcare data, including psychotherapy notes and substance use disorder (SUD) records.
Protecting this data is critical not only to comply with regulations like HIPAA and 42 CFR Part 2 but also to maintain patient trust. With updated 42 CFR Part 2 rules taking effect in February 2026, organizations must meet stricter standards, including breach notification requirements.
Key points include:
Regulatory Compliance: HIPAA and 42 CFR Part 2 set strict guidelines for protecting sensitive data, with penalties for violations reaching $73,011 per violation and up to $2,190,294 annually.
Administrative Safeguards: Appoint security officers, enforce role-based access control, and train staff on security policies and real-world scenarios.
Technical Safeguards: Use AES-256 encryption, multi-factor authentication, and audit logging to secure data at rest and in transit.
Incident Response: Develop a breach response plan, categorize incidents by severity, and notify affected parties within the required timeline.
Physical Security: Secure devices, restrict access to sensitive areas, and use encrypted backups to prevent data loss.
42 CFR Part 2 Compliance: Track consent, flag SUD records digitally, and monitor access to ensure compliance with stricter redisclosure rules.
Administrative Safeguards Checklist
Administrative safeguards are the backbone of any data security program.
While technical measures are essential, they can't fully protect sensitive information without clear policies and procedures to ensure accountability and consistency.
Security Roles and Responsibilities
Start by appointing a HIPAA Security Officer and a Privacy Officer, or combine the roles for smaller organizations [1]. These individuals are responsible for overseeing security policies and ensuring they're consistently applied throughout the organization. They act as the go-to contacts for any security-related issues.
It's also critical to implement role-based access control (RBAC), which limits data access based on job responsibilities [1][4]. For instance, a front desk staff member doesn’t need access to psychotherapy notes, and a billing specialist shouldn’t view clinical assessments.
This aligns with the "minimum necessary" principle, which reduces unnecessary access and limits potential risks. To reinforce this, sanction policies must be in place to address security violations [5]. Without clear consequences, policies risk being ignored.
HIPAA also mandates that organizations retain all security policies, training records, and risk assessments for a minimum of six years [1]. This documentation is critical for demonstrating compliance during audits or breach investigations. Additionally, organizations must execute Business Associate Agreements (BAAs) with any vendor handling PHI, such as EHR providers, billing companies, or cloud storage services [1].
Assigning clear roles is just the first step. To ensure data security, these responsibilities must be paired with effective training.
Staff Training and Awareness Programs
Even the best policies fall short without proper staff training. Security training should begin during onboarding and continue annually [1]. To be effective, training needs to focus on real-life situations and practical examples.
"Security fails when people don't understand why controls exist. Training should be practical and tied to real scenarios your team faces" [4].
Tailor training to the specific challenges of behavioral health.
For example, teach staff how to identify phishing emails targeting therapy records, walk them through the correct way to share progress notes with referring physicians, and show them how to verify a patient’s identity before discussing treatment over the phone.
These realistic examples help employees recognize risks and respond appropriately.
Training should also cover insider threats, which can range from intentional misuse to accidental mistakes. For instance, if a clinician emails a treatment plan to their personal account to finish notes at home, they unintentionally create a security risk.
Awareness programs must stress how behavioral health data breaches can have serious consequences, potentially affecting a patient’s job, family relationships, or safety.
Technical Safeguards Checklist
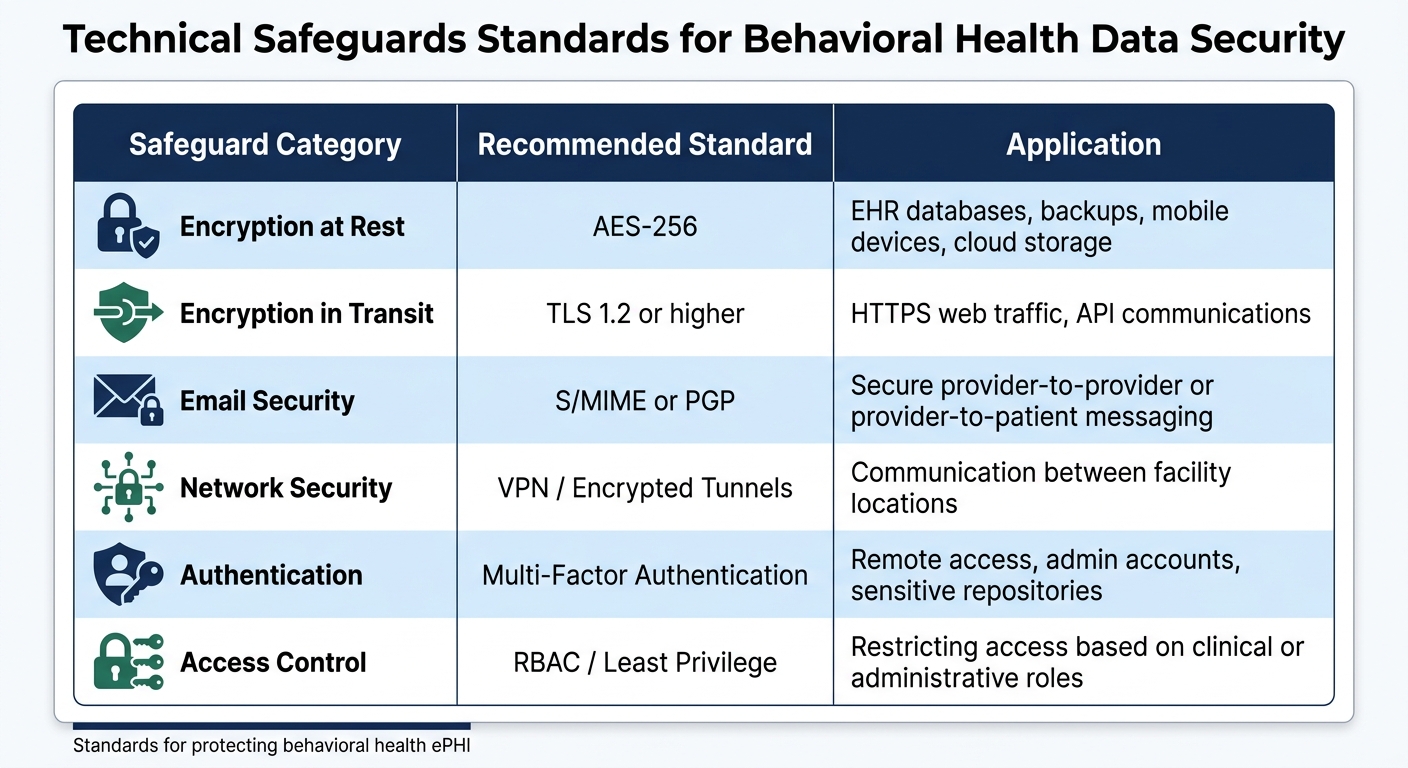
Technical Safeguards Standards for Behavioral Health Data Security
While administrative policies set the groundwork, technical safeguards actively shield electronic protected health information (ePHI) from unauthorized access.
These technology-based measures create multiple layers of defense, significantly reducing the risk of breaches. Here, we’ll explore how encryption, access controls, and audit logging work together to protect sensitive healthcare data.
Encryption and Data Protection
Encryption transforms data into a format that can only be read with the correct decryption key, making it a cornerstone of healthcare data security.
As Calmops explains:
"Encryption is the foundation of healthcare data protection. It ensures that even if data is stolen, it cannot be read without the encryption key." [6]
For stored data - like databases, backups, workstations, and mobile devices - AES-256 encryption is the industry standard. Data in transit, such as web-based communications and API interactions, should be secured using TLS 1.2 or higher.
Proper key management is also essential: encryption keys should be stored separately using methods like Hardware Security Modules (HSMs) or cloud-based Key Management Services (KMS). Rotate keys at least once a year or whenever there are staffing changes.
When sending highly sensitive information, such as treatment summaries, use secure email protocols like S/MIME or PGP. For connecting multiple locations, Virtual Private Networks (VPNs) or encrypted tunnels are vital to protect inter-facility communications.
Considering the high value of medical records on the dark web, encryption is not optional - it’s essential. Once data is encrypted, controlling who can access it becomes the next critical step.
Access Controls and Authentication
Access controls are the gatekeepers of sensitive data, ensuring only authorized individuals can view or modify it. Assign unique login credentials to every staff member and service account - shared accounts and passwords should be eliminated.
Strengthen security further by implementing multi-factor authentication (MFA) for remote access, administrative accounts, and repositories holding sensitive data.
Session security is another key area. Use automatic logouts after inactivity and just-in-time elevation for administrative tasks, granting higher-level permissions only when necessary. Emergency access should follow defined "break-the-glass" protocols, with every instance documented and reviewed afterward.
Regularly review user access rights- at least quarterly - and immediately deactivate accounts when roles change or employees leave. These measures lay the foundation for effective audit logging and monitoring.
Audit Logging and Monitoring
Audit logs serve as a permanent record of who accessed data and when, along with any administrative actions taken. This is not only a security best practice but also a regulatory requirement - HIPAA mandates retaining these logs for at least six years [6].
"Auditability is a security feature, not a compliance afterthought." - Dharmesh Patt, CTO, EvinceDev [4]
An effective logging system should capture critical details, including user access (who accessed what and when), administrative actions (e.g., configuration changes, account updates), and security events (e.g., failed login attempts, emergency access).
Each log entry should include the timestamp, user ID, action performed, patient identifier, resource accessed, and the outcome.
Beyond collecting logs, enable real-time alerts to flag suspicious activity, such as repeated failed logins or unusual access patterns. AI-driven tools can help identify anomalies, while encrypting and restricting access to logs ensures their integrity. Regularly test the logging system to confirm it provides the data needed for thorough incident investigations.
Platforms like Opus Behavioral Health EHR offer built-in audit logging and monitoring tools tailored for behavioral health compliance, simplifying the tracking of access to sensitive therapy and substance use disorder (SUD) records.
|
Safeguard Category |
Recommended Standard |
Application |
|---|---|---|
|
Encryption at Rest |
AES-256 |
EHR databases, backups, mobile devices, cloud storage |
|
Encryption in Transit |
TLS 1.2 or higher |
HTTPS web traffic, API communications |
|
Email Security |
S/MIME or PGP |
Secure provider-to-provider or provider-to-patient messaging |
|
Network Security |
VPN / Encrypted Tunnels |
Communication between facility locations |
|
Authentication |
Multi-Factor Authentication |
Remote access, admin accounts, sensitive repositories |
|
Access Control |
RBAC / Least Privilege |
Restricting access based on clinical or administrative roles |
Incident Response and Breach Management
Even the best security measures can’t stop every breach. When a breach does happen, what matters most is how quickly and effectively you respond. In 2024, the U.S.
Department of Health and Human Services reported over 700 data breaches, impacting nearly 200 million people [19]. For behavioral health organizations managing sensitive therapy notes and substance use disorder (SUD) records, having a solid incident response plan isn’t just a regulatory requirement - it’s essential for maintaining patient trust.
Creating an Incident Response Plan
A well-thought-out incident response plan starts long before a breach occurs. The first step? Build your response team. This team should include breach notification experts, IT security staff, legal advisors, insurance providers, and HR representatives [8].
Make sure critical resources like technical diagrams, vendor contracts, and contact lists are easily accessible when needed.
Detection and reporting are your front-line defenses. Encourage employees to report suspicious activity immediately without fear of punishment. Why is this so important? Around 40% of IT security incidents go unreported because employees worry about repercussions [7].
To address this, consider setting up an anonymous reporting system to make early detection more likely [7]. Remember, the clock starts ticking as soon as there’s reasonable certainty of a breach - not after a full investigation [18].
"Breach notification should be addressed as an integral element of incident response planning, rather than an add-on or afterthought." – Kroll [8]
Once a breach is detected, conduct a risk assessment to determine if it requires notification. This involves analyzing the type of data involved, who accessed it, whether it was actually viewed or acquired, and how much risk has been mitigated [11][12][13][14].
Categorize incidents by severity - low, medium, or high - to allocate resources effectively [9].
Containment is key: take affected systems offline immediately to prevent further data loss while preserving evidence for forensic analysis [17]. Revoke unauthorized access and isolate compromised accounts to stop additional damage [9].
After containing the breach, conduct a "lessons learned" review to address root causes. These reviews often highlight areas needing improvement, like password policies or multi-factor authentication (MFA). Test your plan annually with tabletop exercises and breach response drills to uncover gaps before a real incident happens [9].
Once you’ve contained the breach and started your analysis, the next critical step is timely and compliant breach notification.
Breach Notification Requirements
Effective breach notification builds on your incident response efforts.
Behavioral health organizations face strict requirements under both HIPAA and 42 CFR Part 2. Under HIPAA, breaches affecting 500 or more individuals must be reported to the affected individuals and the HHS Office for Civil Rights (OCR) within 60 days of discovery [7][8].
For smaller breaches (fewer than 500 people), you’ll need to log the incident and report it to HHS within 60 days after the calendar year ends [8]. If a breach impacts more than 500 residents in a single state, you’re also required to notify prominent media outlets within the same 60-day timeframe [11][17].
For SUD records under 42 CFR Part 2, the rules are even stricter. Unauthorized disclosures are automatically considered breaches unless a risk assessment shows minimal impact [12]. Reporting must follow specific workflows and be submitted through the HHS online portal [10][16]. Business associates and Qualified Service Organizations are required to notify the covered entity promptly, but no later than 60 days after discovering the breach.
|
Recipient |
Timeline (Breach ≥ 500 Individuals) |
Timeline (Breach < 500 Individuals) |
|---|---|---|
|
Affected Individuals |
Within 60 days |
Within 60 days |
|
HHS Secretary |
Within 60 days |
Within 60 days after calendar year end |
|
Media Outlets |
Within 60 days |
Not required |
|
Business Associate to Covered Entity |
Within 60 days |
Within 60 days |
Encryption can be your safety net. If data is encrypted or destroyed using HHS-approved methods, notification isn’t required. But if the data wasn’t secured and a breach occurs, your organization must prove the information wasn’t compromised [7].
Sometimes, law enforcement may ask you to delay notifications to avoid interfering with an investigation [7]. Always consult with the FBI or other authorities before proceeding. Finally, ensure you maintain written breach notification policies, train your team, and keep documentation of all assessments and notifications for at least six years [11][15].
Tools like Opus Behavioral Health EHR can simplify compliance tracking and help you stay on top of documentation requirements.
Physical and Facility Security Checklist
When it comes to safeguarding sensitive behavioral health data, physical security is just as important as digital measures. While digital protections often take center stage, a single physical lapse - like an unlocked door or an unguarded laptop - can lead to major data breaches.
Take the case of Parkview Health in June 2014: 71 boxes of medical records, containing information for 5,000 to 8,000 patients, were left in a physician's driveway. This oversight resulted in an $800,000 settlement with the OCR [22]. Physical breaches are not only real but also costly and entirely preventable.
Workstation and Device Security
The placement of workstations plays a crucial role in protecting sensitive information. Screens in high-traffic areas, like waiting rooms or hallways, should be positioned to prevent unauthorized viewing of therapy notes or other private data. Adding privacy filters to monitors in these areas can further reduce the risk of "shoulder surfing" [20].
Hardware security is another key element. Use cable locks to secure desktops and laptops, especially in shared workspaces [20]. For mobile devices, enrolling them in a Mobile Device Management (MDM) system is essential. MDM can enforce full disk encryption, biometric authentication with PINs, automatic timeouts, and remote wipe capabilities [20].
Screen locks and 15-minute inactivity timeouts should be mandatory across all devices to protect data when staff step away [20][21]. Additionally, staff must report lost or stolen devices immediately [20]. Kevin Henry from Accountable emphasizes the importance of encryption:
"Encryption protects confidentiality if a device is lost, stolen, or compromised" [20].
Limit the use of USB drives and other removable media to reduce the risk of data exfiltration. Implement data loss prevention tools to monitor and block unauthorized transfers of PHI [20]. Proper disposal of sensitive data is equally critical - use NIST 800-88-compliant methods for electronic media and cross-cut shredders for paper records [20][21].
A cautionary example: in March 2017, BioReference Laboratories faced repercussions when an employee improperly discarded documents containing PHI for 1,772 patients in a standard dumpster instead of shredding them as required [22].
Once device security is managed, the next step is ensuring data continuity through reliable backup systems.
Backup and Disaster Recovery
Encrypted backups are a must for protecting against ransomware and data loss. Consider the February 2024 breach at Change Healthcare: a $22 million ransom and prolonged system outages left thousands of practices unable to submit claims [21]. Without dependable backups, your organization could face similar disruptions.
To safeguard data, use encrypted backups with strong algorithms like AES-256. Store these backups both offsite and in the cloud, ensuring they are isolated from production systems to prevent ransomware attacks [20].
Recovery keys should be securely stored in a Key Management System (KMS) or Hardware Security Module (HSM) [20]. Regularly test your backup restoration process - quarterly at a minimum - to confirm your disaster recovery plan will work when needed [20][4].
Implement "break-glass" emergency access procedures that allow temporary elevated access during crises, with automatic auditing to track activity [20]. Tools like Opus Behavioral Health EHR can help automate backup tracking and testing schedules, ensuring data stays recoverable.
Finally, control physical access to facilities. Visitor management systems and access controls should restrict entry to areas where sensitive data is stored [20][21].
For staff working from home, their home office is legally an extension of your facility, meaning it must meet the same physical security standards [21].
42 CFR Part 2 Compliance Checklist
As part of safeguarding behavioral health data, compliance with 42 CFR Part 2 introduces additional measures specifically for substance use disorder (SUD) records. These records require protections that go beyond standard HIPAA rules.
The 2024 Part 2 Final Rule brought significant updates, with organizations required to meet full compliance by February 16, 2026 [23][24]. For those who miss the deadline, enforcement by the Office for Civil Rights (OCR) includes penalties tailored to 42 CFR Part 2 violations.
One of the key updates simplifies the consent process, allowing a single consent option for treatment, payment, and health care operations (TPO).
However, organizations must still ensure rigorous tracking and implement segregation measures. Each disclosure requires a redisclosure notice, and unauthorized use of SUD records carries serious consequences - up to $250,000 in fines and 10 years of imprisonment for knowing misuse [2].
SUD Records Segregation
The 2024 rule eliminates the need for physical separation of SUD records. Andrew Zellers from ChartRequest explains:
"HHS also clarified that segregating or segmenting
42 CFR Part 2 data is not required"[24].
Instead of separate databases, organizations can use digital flags within their EHR systems to identify 42 CFR Part 2 data [24][25].
These flags help prevent unauthorized redisclosure during regular HIPAA-permitted sharing and ensure staff apply the correct rules when processing requests. Systems should also be configured to automatically stop data sharing if consent expires or is revoked [25].
SUD counseling notes, however, require special handling. These notes need separate, specific consent and cannot be included under general TPO authorization [24].
Similar to HIPAA psychotherapy notes, they should be kept separate from general medical records.
Once SUD-specific data is flagged digitally, organizations must focus on tracking consent and monitoring access to ensure further protection.
Consent Tracking and Access Auditing
To meet compliance, valid consent forms must include specific details such as the patient’s name, the disclosing program, the recipient’s name or class, the purpose of the disclosure, the information being shared, expiration details, revocation language, and the patient’s signature [2][25].
Additionally, each disclosure must include this notice: "42 CFR part 2 prohibits unauthorized use or disclosure of these records" [24].
Organizations must maintain detailed audit trails to track all access to SUD records. These trails should document who accessed the records, when, and why, including emergency "break-glass" scenarios unique to Part 2 requirements [25]. All compliance-related documentation - including policies, consents, and breach analyses - must be retained for at least 6 years [25].
If acting as an intermediary, such as an ACO or health information exchange, you must provide patients with a list of disclosures made on their behalf over the past three years.
To strengthen security, implement strict role-based access controls using the "minimum necessary" standard. Only staff with a defined clinical or administrative need should have access to SUD-related files [25]. Conduct regular internal audits focusing on SUD disclosures to identify unusual access patterns or missing redisclosure notices [25].
Finally, update Business Associate Agreements and Qualified Service Organization Agreements to include Part 2-specific language addressing redisclosure limits and incident response procedures [25].
Documentation and Continuous Improvement
Strong technical and administrative safeguards are only part of the equation when it comes to compliance - consistent documentation and regular reviews are equally critical. Documentation isn't just about meeting requirements; it's the backbone of a defensible compliance strategy. Without clear and detailed records, organizations may struggle to demonstrate their efforts to protect patient data, leaving them exposed during audits or investigations.
Required Documentation and Records
HIPAA requires organizations to retain compliance documentation for at least six years [3]. This includes written policies addressing the Privacy Rule, Security Rule, and Breach Notification Rule, as well as records like risk assessments, training logs, and signed Business Associate Agreements (BAAs) for all third-party vendors [3].
The Office for Civil Rights (OCR) takes missing or incomplete risk assessments seriously, often treating them as major HIPAA violations [3].
Operational logs are another essential piece. These logs should track system activity, including who accessed records and when. Incident response logs are also crucial for documenting security events or breaches [3][4].
For behavioral health providers managing substance use disorder data, additional documentation like consent forms and re-disclosure notices must meet both HIPAA and the stricter 42 CFR Part 2 requirements [3]. Audit-ready documentation is a powerful tool for compliance.
The stakes are high - penalties can reach $73,011 per violation, with an annual cap of $2,190,294 [3]. Detailed training records, including attendance, dates, and competency evaluations, can show that your organization takes security seriously [3].
Beyond compliance, thorough documentation supports proactive security measures and lays the groundwork for ongoing audits.
Regular Risk Assessments and Audits
Compliance is not a one-and-done task; it's an ongoing process. As Dharmesh Patt, CTO at EvinceDev, puts it:
"Compliance isn't a one-time release activity; it's a continuous operational discipline." [4]
Risk assessments should be conducted at least once a year and whenever significant changes occur, such as new integrations, major software updates, or adjustments to data pipelines [3][4].
Daily monitoring is equally important, especially in behavioral health software environments. AI-driven tools can be invaluable here, identifying unusual access patterns or suspicious login attempts in real time - something manual reviews might miss [4].
Organizations that can show a track record of recognized security practices for at least 12 months may benefit from leniency during OCR enforcement actions [5].
Additionally, regularly testing backup restores ensures recovery procedures work as intended [4]. Reviewing access logs can help catch configuration issues, and re-testing security measures after system updates keeps defenses sharp [4].
By turning compliance documentation into a living, proactive resource, organizations can stay ahead of risks and maintain a strong compliance posture.
Conclusion and Key Takeaways
Protecting data in behavioral health isn't just a good practice - it's essential for safeguarding both your patients and your organization. The consequences of neglect are severe: as of 2026, HIPAA penalties for willful neglect start at $73,011 per violation, with annual caps reaching $2,190,294 per violation category [1].
Beyond financial penalties, breaches can lead to criminal charges, including fines up to $50,000 and even imprisonment for up to one year for knowingly misusing protected health information [1]. Start by assigning a HIPAA Security Officer and Privacy Officer, conducting a thorough risk assessment (a critical requirement emphasized by the Office for Civil Rights), and establishing Business Associate Agreements with all vendors handling patient data [27].
Since human error or misconfigurations account for 95% of data breaches, addressing these vulnerabilities is a top priority [27]. On the technical side, safeguard sensitive information with tools like Multi-Factor Authentication, role-based access controls, and encryption for both data at rest and in transit [4].
Physical security also demands attention - more than 22% of breaches still involve paper records [26]. Simple measures like positioning monitors out of public view, requiring visitor sign-ins, and securely disposing of physical documents can make a big difference.
For organizations handling substance use disorder records, compliance with both HIPAA and 42 CFR Part 2 is critical. The 2024 updates to Part 2 have simplified some consent requirements while maintaining strict rules against re-disclosure and offering heightened protections [1].
Compliance should be seen as an ongoing responsibility, not a one-time task. Be sure to retain all documentation for the required six-year period [3].
Adopting recognized security practices consistently for at least 12 months can also result in more favorable enforcement outcomes from the OCR [5].
Combining strong administrative, technical, and physical measures creates a comprehensive security framework. By following these steps, you not only ensure compliance but also strengthen patient trust and confidence in your organization.
FAQs
What changes do we need to make before 02/16/2026 for 42 CFR Part 2?
By February 16, 2026, organizations are required to revise their Notices of Privacy Practices and internal policies to align with the updated 42 CFR Part 2 regulations.
This involves ensuring that all confidentiality and consent requirements are fully addressed to meet the compliance deadline.
How can we prove 'minimum necessary' access with RBAC and audit logs?
Proving "minimum necessary" access involves implementing role-based access controls (RBAC) to ensure users only have permissions aligned with their specific job duties. Additionally, maintaining comprehensive audit logs is crucial.
These logs document who accessed what and any changes made, providing a clear trail for compliance and accountability. By combining RBAC with detailed logging, organizations can effectively meet data security standards while safeguarding sensitive information.
What should our breach response plan include to meet HIPAA and Part 2 deadlines?
Your breach response plan needs to detail specific steps to meet HIPAA and Part 2 deadlines.
This means notifying affected individuals, the Department of Health and Human Services (HHS), and any other relevant authorities within the required timeframes.
It's also critical to keep thorough records of all breach response actions to ensure compliance.
