Timing is extremely essential in healthcare. If feedback comes in too late, it can’t change care.
In behavioral health, the best tools send patient input during treatment or right after a visit, route low scores to the right staff, and log follow-up in the chart.
That matters because SMS response rates can hit 30%–50% in rehab and SUD settings, while paper surveys may get only 5%–10%, and 96% of unhappy patients never complain directly.
What to focus on:
Use case: feedback collection, symptom tracking, or formal measurement-based care
Timing: intake, 72 hours after admission, mid-treatment, end of session, discharge
Delivery: SMS, app links, QR codes, tablets, telehealth check-ins, EHR prompts
Clinical use: PHQ-9, GAD-7, alliance tools, trend lines, risk alerts
Workflow: who gets alerts, who calls the patient, and who documents follow-up
Privacy: HIPAA, 42 CFR Part 2, audit trails, and neutral SMS wording
System fit: EHR sync, auto-scoring, milestone triggers, and closed-loop follow-upA feedback tool only helps if staff can act on the data while care is still in progress. Used well, these tools can help teams spot relapse risk, fix service issues within 24 hours, and improve outcomes by 10% to 20%.
What These Tools Do and Why Practices Use Them
Once a practice knows when to ask for feedback, the next step is simple: figuring out how to put that feedback to work. These tools send patient input to the right people fast enough to affect care, follow-up, or day-to-day operations.
Common Feedback Workflows and Tool Types
Practices collect feedback at several points across the patient journey.
Common touchpoints include in-office tablets or kiosks, QR codes in waiting rooms, automated SMS prompts, secure telehealth links, and EHR-integrated check-ins.
Each option fits a different moment. Teams often use SMS or secure links for intake, midpoint, and discharge feedback, depending on the care setting. End-of-session tools like the Session Rating Scale focus on the therapeutic relationship, which gives clinicians a way to spot alliance ruptures early. The best workflow depends on the goal: clinical monitoring, patient engagement, or service recovery.
Benefits for Clinical Care, Patient Engagement, and Operations
Steady feedback helps clinicians spot problems they might not catch otherwise. Andrea Horwitz, Clinical Director at Opus Behavioral Health, shared this example:
"Reviewing weekly treatment results shows me what is really happening with my clients, even if they are not able to express it in session... We were able to work together to prevent a relapse, a crisis, and potential tragedy." [1]
That kind of visibility matters.
Nearly 96% of unhappy patients never complain directly; they simply leave or do not return [6]. In plain terms, silence doesn't mean things are fine.
Automated pulse checks help teams find service, facility, and support issues early. When a low score comes in, the system can send an alert to a clinical director or operations manager so someone can step in fast, often within 24 hours [2].
There’s another practical upside. High scores can guide patients toward public reviews, while low scores stay in an internal recovery channel. That gives practices a cleaner way to handle praise and problems without relying on manual follow-up. It also creates a steady contact record for audits and reviews [2].
And this isn't just about smoother operations. Real-time feedback has been shown to improve treatment outcomes by 10% to 20% [7].
The same data can then shape workflow, documentation, and escalation rules.
How to Evaluate a Real-Time Feedback Platform
Once your feedback workflows are mapped out, the next step is simple: make sure the platform can handle them without piling more work onto staff.
A lot of feedback tools fall short in behavioral health. The goal is to pick a system that fits clinical work as it already happens, not one that forces teams into extra manual tasks.
Clinical and Workflow Fit
Start with one core question: does the platform support measurement-based care (MBC)?
Look for tools with preloaded, auto-scored assessments like PHQ-9 and GAD-7, along with trend graphs that let clinicians spot change over time without digging through raw data.
A good platform also automates feedback requests at set clinical milestones, instead of making staff remember to send reminders by hand [2].
Escalation paths matter too. If a patient reports a low score, the system should trigger immediate alerts and document follow-up in a closed loop inside the EHR. That kind of setup cuts down on missed steps and keeps the response tied to the care record.
Integration, Analytics, and Compliance Requirements
If a tool lives outside the EHR, it creates friction fast. Survey scores should flow straight into the patient's chart through direct EHR integration, so feedback stays part of care instead of getting stuck in a separate silo.
In behavioral health, privacy and security aren't add-ons. They're part of basic platform fit. Check for HIPAA, 42 CFR Part 2, Joint Commission, and CARF alignment, along with MFA, encryption, and audit trails [4]. SMS design matters as well. Messages should avoid naming the facility type, which helps lower the chance of exposing a patient's treatment status if someone else sees the phone screen [5].
Clinical data only helps if staff can see it where they already do their work.
|
Evaluation Category |
Key Requirements to Verify |
|---|---|
|
Compliance |
HIPAA, 42 CFR Part 2, Joint Commission/CARF alignment, audit trails |
|
Integration |
Open APIs, HL7 standards, automated EHR data sync |
|
Security |
MFA, data encryption (at rest and in transit), secure SMS |
|
Clinical Fit |
Customizable assessments (PHQ-9/GAD-7), tiered alerts, trend visualization |
|
Workflow |
Milestone-based triggers, real-time staff notifications, QR code support |
Opus Behavioral Health EHR supports outcomes measurement, automated workflows, reporting, telehealth, and behavioral health compliance needs [1] [4].
After selection, workflow ownership and response rules determine whether the system delivers value.
How to Implement Real-Time Feedback Tools
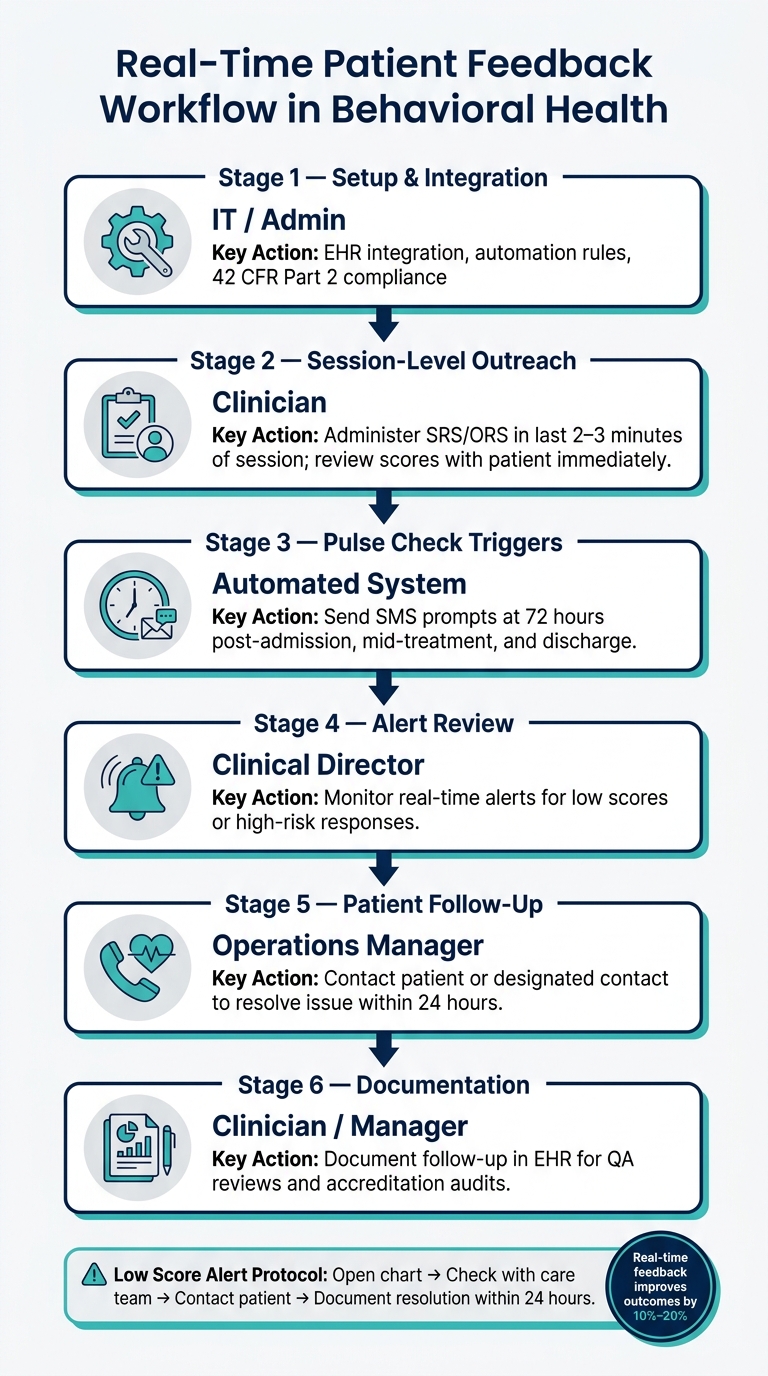
Real-Time Patient Feedback Workflow in Behavioral Health
Set Up Workflow Ownership, Patient Consent, and Response Rules
After you pick a platform, set ownership and response rules before the first patient message goes out.
If no one owns the workflow, things bog down fast. Prompts sit there. Alerts get missed. Feedback ends up doing nothing.
Here’s a simple way to split the work across your team:
|
Workflow Stage |
Primary Owner |
Key Responsibility |
|---|---|---|
|
Setup & Integration |
IT / Admin |
EHR integration, automation rules, and 42 CFR Part 2 compliance [7][5] |
|
Session-Level Outreach |
Clinician |
Administering SRS/ORS in the last 2–3 minutes of each session and reviewing scores immediately with the patient [7] |
|
Pulse Check Triggers |
Automated System |
Sending SMS prompts at 72 hours post-admission, mid-treatment, and discharge [2] |
|
Alert Review |
Clinical Director |
Monitoring real-time alerts for low scores or high-risk responses [2] |
|
Patient Follow-Up |
Operations Manager |
Contacting the patient or designated contact to resolve the issue [2] |
|
Documentation |
Clinician / Manager |
Consent matters too. Patients should know from the start if they may get digital check-ins and whether messages go to the patient, a family contact, or both. SMS prompts should use the practice name only.
They should avoid terms like "substance use" or "behavioral health" in the message text to protect privacy and align with 42 CFR Part 2 [5].
When a low score comes in, speed matters. Send alerts to clinical directors or operations managers by SMS or push notification right away [2].
The aim is to close the loop within 24 hours with a simple three-step recovery: open the patient’s chart, check with the care team, then contact the patient or designated contact to resolve the issue [2]. Every fix should be documented in the patient’s chart for QA reviews and accreditation audits [1][2].
Train Staff and Connect Feedback to Treatment Decisions
Once ownership and alerts are in place, train staff to use trends in care decisions, not just glance at scores.
A single PHQ-9 or GAD-7 score gives you a snapshot. A pattern over several sessions tells you where care may need to change. If scores improve over time, that points in one direction. If they flatten for weeks, that points somewhere else.
Use outcome data for peer coaching and to spot what’s working across the team, not as a staff scorecard. People tend to buy in when they can see feedback leading to actual care changes, like adjusting session frequency or updating treatment goals. Leadership should pull monthly data and share team-wide trends so everyone can see the same picture.
This data should also shape day-to-day operations. Mid-treatment score patterns can help flag patients who may be at risk of leaving against medical advice. When feedback ties into decisions staff already make, it stops feeling like one more task dumped on the pile.
Common Implementation Mistakes to Avoid
Even a good tool can fall apart if alerts have no owner or no response rule.
Treat every low response like an action item, not just another number on a dashboard. The whole point is to get the data to someone who can act on it.
Two mistakes show up again and again:
No action plan for high-risk responses: If a patient flags distress or shows suicidal ideation, the system needs a critical alert that requires a documented response.
Disconnected data: If feedback sits outside the EHR, it turns into a silo. Scores that don’t sync to the patient chart can’t guide treatment decisions or support audit requirements.
Opus Behavioral Health EHR supports outcomes measurement and automated workflows that keep feedback tied to the chart.
Conclusion: Building a Feedback Process That Improves Care
Real-time feedback improves care only when a practice connects standardized measurement with clear follow-up. The strongest programs use standardized assessments at set milestones like intake, mid-treatment, and discharge [3]. They also have plain rules for who steps in when a low score comes in.
This works best when scores show up right in session notes, so clinicians can respond without leaving the chart [3]. Clear ownership, documented follow-up, and staff training help turn scores into action [3]. Weekly outcome data can also surface things patients may not say out loud during a session.
Opus Behavioral Health EHR supports outcomes measurement, automated workflows, and reporting tools, so feedback stays tied to the chart. When measurement, routing, and follow-up work together, feedback helps care instead of adding more work.
FAQs
How do real-time feedback tools fit into daily clinical workflows?
Real-time feedback tools work best when they slide into everyday clinical workflows. They track patient data and bring useful next-step insights straight into the electronic health record, so clinicians can act without jumping between systems.
Opus Behavioral Health EHR does this by automating patient-reported outcomes and assessments, sending results to the care team right away, and triggering alerts when critical changes show up. That gives clinicians a clear signal to adjust treatment plans in real time.
What should we look for before choosing a feedback platform?
Look for a platform that fits the workflows and EHR you already use, supports real-time feedback while patients are still in your care, and works well for behavioral health needs like outcome measurement and compliance.
It also helps to look at the vendor’s training and support. And don’t settle for a platform that only gives you star ratings. You want data your team can actually use for quality control. Opus Behavioral Health EHR includes outcomes measurement and AI-powered tools.
How can practices respond quickly to low or high-risk scores?
Practices can use Opus Behavioral Health EHR to react fast to risk scores. When patients finish assessments, the system calculates scores on its own and sends instant alerts to the care team when a critical threshold is reached.
Clinicians can then check results in clinical dashboards and step in right away. That might mean addressing high-risk patterns or an emotional crisis, updating the treatment plan, or setting up extra sessions to support patient safety and outcomes.
