
APIs are transforming how behavioral health providers share patient data, replacing outdated methods like faxes and phone calls with automated, real-time exchanges.
They connect systems like EHRs, labs, and pharmacies, ensuring clinicians have accurate, up-to-date information for better decision-making.
Key benefits include:
Improved Data Sharing: APIs enable seamless transfer of demographics, lab results, medications, and care plans.
Enhanced Care Coordination: Providers can instantly share referrals, treatment notes, and crisis plans.
Compliance with Standards: APIs built on FHIR and USCDI v3 ensure alignment with federal regulations.
Time Savings: Automating workflows reduces administrative burdens, freeing up staff to focus on patient care.
APIs not only streamline operations but also improve patient safety by reducing errors and ensuring continuity of care during transitions. With new regulations in 2026, adopting API-driven systems is essential for modern behavioral health organizations.
APIs in Behavioral Health: Key Stats & Benefits at a Glance
How APIs Support Behavioral Health Data Exchange
An Application Programming Interface (API) acts as a bridge between different systems, enabling them to communicate seamlessly.
For example, when a lab sends toxicology results to an EHR or a billing platform retrieves a patient’s insurance details, an API handles these tasks automatically in the background.
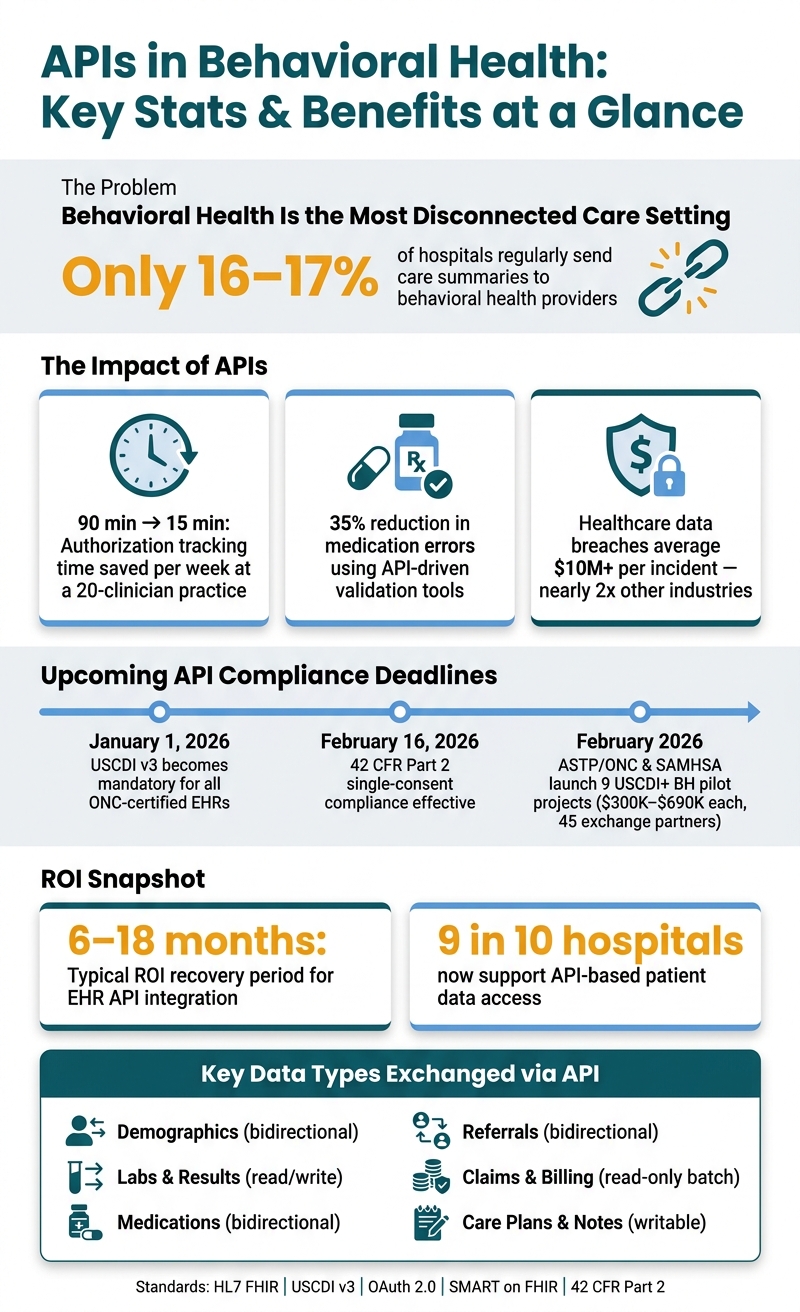
In the behavioral health field, this capability is especially critical. Shockingly, only 16–17% of hospitals regularly send care summaries to behavioral health providers, the lowest rate among all care settings [4]. APIs step in to create dependable, automated pathways that deliver the right data to the right place at the right time.
Key Data Types in Behavioral Health
Behavioral health organizations manage a variety of sensitive data types that need to move accurately between systems. Below is a breakdown of the most common data types, how APIs facilitate their flow, and the impact on workflows:
|
Data Type |
API Direction |
Workflow Impact |
|---|---|---|
|
Demographics |
Bidirectional |
Prevents duplicate data entry during intake processes. |
|
Labs & Results |
Read/Write |
Provides near-real-time access without manual chart pulls. |
|
Medications |
Bidirectional |
Helps prevent drug interactions and supports e-prescribing. |
|
Referrals |
Bidirectional |
Speeds up admissions and reduces manual handoffs. |
|
Claims & Billing |
Read-only (Batch) |
Reduces claim denials and accelerates reimbursement cycles. |
|
Care Plans & Notes |
Writable |
Ensures therapists and prescribers are aligned on treatment plans. |
By streamlining these data exchanges, APIs ensure that clinicians always have access to the most up-to-date information.
This doesn’t just apply to external data sharing; APIs also enhance internal interoperability, allowing, for instance, a therapist and psychiatrist within the same facility to access shared treatment plans and crisis notes instantly [4].
These automated data flows replace outdated processes, saving time and improving care quality.
How APIs Replace Manual Data Sharing
Before APIs became widespread, behavioral health staff often relied on fax machines, scanners, and phone calls to exchange patient information.
This manual approach introduced inefficiencies and created gaps in clinical records, as the same information had to be entered into multiple systems. This left clinicians with an incomplete view of patient care.
"A prescriber who can't see a patient's full medication history is making decisions with incomplete information. That's a patient safety problem." - The PIMSY Team [4]
A great example of API-driven transformation comes from MHCD, which adopted an API-first approach in 2020 using Microsoft Azure.
By September, they had launched a telehealth app and integrated DocuSign for remote paperwork. By December, they added an API to manage patient engagement goals [3].
This shift from manual processes to automated, API-driven systems allowed the organization to act quickly, reduce administrative burdens, and keep all systems aligned with patients' evolving needs.
API Standards and Interoperability Models
When it comes to automated data exchanges, having solid API standards is key to making sure systems can communicate effectively. It’s not just about transferring data - it’s about ensuring that the systems exchanging the data interpret it in the same way, especially when it comes to its clinical meaning [1].
FHIR and HL7 Standards in Behavioral Health
HL7 FHIR (Fast Healthcare Interoperability Resources) has become the go-to standard for modern health data exchange. Unlike older HL7 v2 formats, FHIR uses a RESTful, resource-based framework similar to how the web operates. This makes it faster to implement and easier to maintain.
To better address mental health and substance use disorder (SUD) care, the Office of the National Coordinator for Health IT (ONC) and SAMHSA introduced the USCDI+ Behavioral Health (USCDI+ BH) dataset.
Built on FHIR, this specialized guide is tailored to the unique needs of behavioral health [2][7]. By January 1, 2026, all ONC-certified EHRs are required to support USCDI Version 3, which includes new data classes like mental and cognitive status, pregnancy status, and disability status [4].
The table below highlights how USCDI versions have expanded to include behavioral health elements:
|
USCDI Version |
Key Behavioral Health Elements Added |
|---|---|
|
Version 2 |
SDOH Assessment, Goals, Problems, and Interventions |
|
Version 3 |
Mental/Cognitive Status, Pregnancy Status, Disability Status |
|
Version 4 |
Alcohol Use, Substance Use, Physical Activity |
These evolving standards are already making an impact. For instance, platforms like CalMHSA Connex are leveraging HAPI FHIR and HL7 FHIR standards to securely share treatment plans and outcomes across 24 California counties, including San Diego and Sonoma.
This platform also handles complex privacy and consent protocols [8].
In February 2026, ASTP/ONC and SAMHSA launched nine pilot projects to test the USCDI+ BH dataset and FHIR Behavioral Health Profiles Implementation Guide.
These projects, involving 45 exchange partners across states like Colorado, Connecticut, and North Carolina, received funding between $300,000 and $690,000 each. They focus on real-world scenarios like care coordination and consent management [2].
Actionable Tip: Make sure your EHR vendor is ONC-certified. This ensures that their system supports FHIR APIs and complies with USCDI Version 3 requirements [4].
Authentication and Security Protocols
Defining data standards is just one piece of the puzzle - securing those exchanges is just as critical. While FHIR specifies what data is exchanged, security protocols determine who can access it and how it’s protected.
The most commonly used framework for this is OAuth 2.0, often paired with SMART on FHIR, to manage third-party app access to patient data [6].
For secure API connections, organizations should use TLS 1.2 (or higher) for data in transit and AES-256 encryption for data at rest [6].
Additionally, Role-Based Access Control (RBAC) ensures that staff only access the minimum necessary PHI for their roles. Maintaining immutable audit logs - which track data access and changes - helps meet CARF and Joint Commission compliance requirements [6].
Before connecting any external system via API, organizations should request these three critical documents from their vendor:
A signed Business Associate Agreement (BAA)
A SOC 2 Type II report
A penetration test summary from the past 12 monthsThese documents confirm that the vendor’s security measures have been reviewed and independently verified [6].
How APIs Are Used in Behavioral Health Settings
APIs are transforming how behavioral health organizations operate by streamlining processes and improving data flow. By adhering to established standards and security protocols, they enable seamless system integrations that directly impact patient care.
EHR-to-Lab Integration
Lab results in behavioral health aren't just routine - they're crucial for guiding treatment. For example, clinicians may rely on lab data to monitor lithium levels for patients with bipolar disorder or to track drug use patterns in a substance use disorder (SUD) program.
APIs bridge the gap between Electronic Health Records (EHRs) and Laboratory Information Systems (LIS), allowing these systems to communicate effectively, even when they use different protocols [9][10].
The impact? Lab results are delivered directly to the EHR as soon as they're available. No more logging into separate systems or manually retrieving data.
Clinicians can access everything they need from one interface, leading to faster decisions and reducing the risk of errors. This streamlined process also lays the groundwork for improved medication management.
E-Prescribing and Medication Management
Managing medications in behavioral health is a high-stakes task. APIs give clinicians a real-time view of a patient's medications, pulling data from pharmacies, previous EHRs, and Prescription Drug Monitoring Programs (PDMPs) all at once [1][12].
This is especially critical for SUD treatment, where APIs enable Electronic Prescribing of Controlled Substances (EPCS).
By simplifying the process of prescribing medications like buprenorphine, APIs help providers stay compliant with federal regulations while reducing administrative hurdles [1][4].
Modern APIs built on FHIR standards use the MedicationRequest resource to organize this data, ensuring it's actionable and easy to understand across systems [6].
They also support closed-loop medication management, where prescription updates and pharmacy fulfillment details automatically sync back to the patient’s primary record [11].
One key point to consider: when integrating systems bidirectionally, it’s important to designate a single source of truth for high-risk medication orders. This avoids conflicting updates when data flows from multiple sources [6].
Referral and Care Coordination
Referrals are often a bottleneck in behavioral health. APIs simplify this process by enabling real-time, two-way exchanges of referral data between systems.
This means psychiatrists, therapists, and primary care doctors can share crisis plans, treatment notes, and medication lists instantly - without relying on phone calls or faxes. By eliminating these manual steps, APIs reduce delays, ensure continuity of care, and keep patient records unified.
Steps to Implement APIs in Behavioral Health Organizations
Getting API integration right involves more than just connecting systems. It requires careful planning, clear roles, and a step-by-step rollout.
Mapping Systems and Data Needs
Set aside 1–3 weeks for a discovery phase to fully understand your systems and data flows [6]. This involves identifying all existing platforms - like EHR, CRM, RCM, labs, telehealth, and patient portals - and pinpointing where data handoffs are failing [6][13].
A critical decision during this phase is choosing a single system of record for sensitive data, such as medication orders or insurance claims. Without this, bidirectional integrations can lead to conflicting updates, potentially causing clinical errors [6].
While demographic data may be less risky, high-stakes fields like medications, allergies, and care plans require carefully defined reconciliation rules.
"One of the key learning methods is human-centered design. So we talk to folks, we test, we learn and we ask how it's working for people." - Wes Williams, CIO, Mental Health Center of Denver [3]
This human-centered approach is vital. Engaging with clinical and administrative staff to understand where workflows break down ensures that your integrations will simplify processes rather than complicate them [3].
Once systems and data needs are mapped out, move on to thorough testing and monitoring to ensure your APIs perform reliably.
Testing and Monitoring API Performance
After validating your data models in a sandbox environment, begin phased testing. This includes connectivity tests, unit tests, end-to-end tests, and clinical user acceptance testing (UAT) with staff [6].
This stage usually takes 2–6 weeks and should include load testing to confirm that APIs can handle peak usage.
Post-launch, plan for a 30–90 day hypercare period to monitor key metrics like data latency, transaction errors, and reconciliation issues [6].
Use a defined KPI plan to measure success. For example:
|
KPI |
What It Measures |
Target Signal |
|---|---|---|
|
Data Latency |
End-to-end message transfer time |
Sustained reduction from baseline |
|
Error Rate |
Failed transactions by type and source |
Trending toward zero for known errors |
|
Admin Hours Saved |
Staff time per task before vs. after |
Measurable reduction by 90 days |
|
Claim Denial Rate |
Denials tied to integration-related billing |
Declining trend by 90 days |
|
Time to Schedule |
Referral receipt to confirmed appointment |
Decreasing within 30 days |
Always have manual fallback procedures in place for critical data requests during API downtime [6]. Once performance is stable, make these fallback measures part of your standard operations.
Additionally, schedule quarterly reviews to check for vendor API updates or deprecations that could disrupt workflows.
Data Security and Compliance for API Use
Once your APIs are up and running, keeping security and compliance front and center is crucial. Behavioral health data is particularly sensitive, and with the importance of smooth API integration already highlighted, strong security measures are non-negotiable.
The stakes are high - healthcare data breaches now average over $10 million per incident, nearly double the average across industries [16].
HIPAA Compliance and Data Privacy
When it comes to APIs, HIPAA compliance revolves around three key rules: the Security Rule (covering encryption and access controls), the Privacy Rule (limiting data access to the minimum necessary), and the Breach Notification Rule [18][20]. These rules directly shape how APIs should be developed and maintained.
To enforce access control, assign unique API tokens to each user. This creates a clear audit trail and ensures that tokens are restricted to accessing only the data needed for their specific purposes [19].
In behavioral health, 42 CFR Part 2 adds another layer of complexity. For substance use disorder (SUD) records, explicit and detailed patient consent is required before sharing any information - going beyond the standard permissions under HIPAA [21].
Federal mandates require maintaining immutable, tamper-proof audit logs for at least six years [18][20].
And the financial penalties for non-compliance are steep: as of 2025, fines for willful neglect start at $73,011 per violation, with annual caps reaching $2,190,294 [20].
"HIPAA compliance is a floor, not a ceiling." - Dr. Girirajtosh Purohit [16]
Once compliance measures are solid, the next focus is securing data during transmission.
Secure Data Transmission
Beyond encryption basics, behavioral health APIs demand additional safeguards. For highly sensitive data - like psychotherapy notes or HIV status - field-level encryption is essential. This ensures that even if the application layer is breached, the data remains protected [14][16].
When sharing data across organizations, mutual TLS (mTLS) is a must. This protocol ensures that both the client and server authenticate one another, closing off vulnerabilities where malicious actors might impersonate trusted applications [16].
Pairing mTLS with an API gateway adds another defense layer, allowing you to enforce rate limits and detect unusual query patterns, such as bulk data requests [16].
Adopting a Zero Trust Architecture strengthens security further. This approach assumes that no request is inherently safe - whether it originates inside or outside your network.
Each API call must be authenticated and authorized based on factors like identity, device health, and context [15][16].
Adding phishing-resistant multi-factor authentication (preferably FIDO2 hardware keys over SMS codes) significantly reduces risks of account takeovers and unauthorized access [14][15].
Here’s a quick summary of key security layers and their protocols for protecting APIs:
|
Security Layer |
Protocol/Standard |
Purpose |
|---|---|---|
|
Transport Security |
mTLS / TLS 1.2+ |
Encrypts data in transit and ensures endpoint authentication [14][16] |
|
Authorization |
OAuth 2.0 / SMART on FHIR |
Manages granular access permissions and ensures minimal data sharing [16] |
|
Authentication |
MFA (FIDO2/TOTP) / SSO |
Verifies user identity and prevents account takeovers [14][15] |
|
Data Integrity |
AES-256 / HMAC-SHA256 |
Secures data at rest and ensures message authenticity [14][17] |
|
Monitoring |
SIEM / Distributed Ledger |
Provides tamper-proof audit trails and real-time threat detection [14][16] |
Benefits of API-Based Interoperability
When paired with solid security and compliance measures, API-driven interoperability can transform both operational workflows and patient care in meaningful ways.
Faster, More Efficient Workflows
Manual tasks like faxing records, calling pharmacies, or chasing down approvals can eat up hours of valuable time. APIs streamline these processes by enabling automated, real-time data sharing.
Take, for example, a 20-clinician behavioral health practice in Greenville. By implementing an interoperable EHR with API-driven authorization tracking, they reduced the time spent on this task from 90 minutes per week to just 15 minutes [4].
These time savings ripple across other areas like billing, lab work, and referrals.
"What you're doing with APIs is exposing a problem to a solution... utilizing APIs was the way to do that." - Wes Williams, CIO, Mental Health Center of Denver [3]
APIs also address internal inefficiencies by bridging data gaps, allowing real-time updates to flow seamlessly between systems.
Better Patient Outcomes
Operational improvements don’t just save time - they directly enhance patient care. Real-time access to complete data equips clinicians to make quicker, more informed decisions, which is critical in behavioral health.
Medication safety highlights this impact clearly. Practices using API-driven validation tools have seen a 35% reduction in medication errors. This is crucial given that improper medication use in 2022 contributed to approximately 175,000 deaths and 1.25 million serious adverse events in the U.S. [3][23].
APIs enable prescribers to instantly review a patient’s full medication history, including allergy warnings and drug interaction alerts, significantly reducing risks tied to incomplete data.
APIs also play a key role in ensuring continuity of care during transitions, such as moving from detox to outpatient treatment or from an emergency department back to a primary behavioral health provider.
Currently, only 16–17% of hospitals routinely share care summaries with behavioral health providers [22].
APIs help close this gap by automatically transferring patient records, ensuring providers have the information they need.
"Improved electronic data exchange can expand access to behavioral health care, support enhanced care coordination, empower clinical decision-making, and lead to improved health outcomes." - Dr. Thomas Keane, National Coordinator for Health IT [22]
The Mental Health Center of Denver offers a real-world example of these benefits.
Between April and December 2020, they deployed several APIs, including a telehealth app, a DocuSign integration for remote paperwork, and a tool for inter-session engagement.
These tools eliminated logistical barriers like transportation and waiting room delays, allowing patients to progress through treatment more efficiently [3].
Opus Behavioral Health EHR: API-Driven Interoperability
Opus Behavioral Health EHR is purpose-built to integrate clinical, administrative, and billing processes into a unified system. Specifically tailored for mid-sized behavioral health and substance use disorder (SUD) treatment centers, it addresses the needs of an often-overlooked segment in health IT.
By leveraging an API-driven architecture, Opus connects essential workflows, embodying the interoperability advantages discussed throughout this article. Learn more at Opus Behavioral Health EHR.
Key Features That Support Interoperability
Opus employs HL7, FHIR, and RESTful APIs to enable seamless, two-way data sharing across core systems used by behavioral health providers. For instance:
Lab Integration: Direct connections with over 500 diagnostic labs nationwide allow clinicians to order tests and view results directly within patient charts. This eliminates the hassle of juggling multiple logins and reduces manual data entry. Automated alerts for abnormal lab results ensure timely follow-up, improving patient care.
E-Prescribing: Through DoseSpot, clinicians can access real-time drug interaction alerts and complete medication histories, fully integrated with clinical notes. This streamlines prescribing and enhances patient safety.
Telehealth Integration: The telehealth module is embedded within the clinical workflow, allowing video sessions, scheduling, and documentation to occur within a single HIPAA-compliant interface.In March 2026, Opus introduced a secure API integration with Brellium for automated chart reviews. This feature audits session notes against payer requirements before claims submission, reducing documentation errors.
Practices using Brellium through Opus have reported spending 98% less on pre-billing chart reviews and completing session notes 13 times faster than those relying on manual processes [26].
To further support compliance, Opus adheres to USCDI v3 standards and includes tools for managing 42 CFR Part 2 requirements, ensuring sensitive SUD records are handled with enhanced access controls.
How Opus Supports Behavioral Health Operations
The benefits of Opus extend beyond clinical interoperability, offering tools that simplify everyday operations.
In May 2026, Opus partnered with XY.AI Labs, becoming the first platform in its category to integrate AI-driven automation natively.
Through direct API connections and browser-based navigation, this feature automates repetitive tasks like claims management, payment posting, and patient onboarding without requiring custom development.
"The operators we serve are under-resourced and over-burdened. They got into this work to help others, not to spend their days on grunt work. Integrating XY AI's agents directly inside Opus allows our customers to automate the work that has been holding them back and double down on what they do best." - Humberto Buniotto, CEO and Founder, Opus [25]
Additionally, the platform includes Copilot AI, a scribe tool that drafts progress notes for both in-person and telehealth sessions.
This feature reduces documentation time by 40% [24]. For operational and clinical leaders, Opus offers over 140 customizable reporting options to track outcomes, monitor billing performance, and identify care gaps.
These API-enabled features demonstrate how interoperability can enhance care delivery and operational efficiency, ultimately benefiting both providers and patients alike.
Conclusion: The Case for APIs in Behavioral Health
Behavioral health has historically been one of the most disconnected areas in healthcare. For instance, only 16–17% of hospitals regularly send care summaries to behavioral health providers - the lowest rate among all care settings [4]. APIs offer a direct solution to this problem by replacing outdated tools like fax machines and manual data entry with real-time, standards-based data sharing.
The benefits are undeniable. Organizations that adopt an API-first approach not only streamline their technology but also improve their ability to respond quickly.
As Wes Williams, CIO of the Mental Health Center of Denver, aptly said:
"In behavioral healthcare, the biggest problem is access to care... technology can act as a force multiplier, automating previously manual operations." [3]
This "force multiplier" effect is transformative. For example, manual tasks like authorization tracking can shrink from 90 minutes to just 15 minutes [4].
Additionally, organizations often recover their investment in EHR integration within 6 to 18 months [6]. With 9 in 10 hospitals now supporting API-based patient data access [5], the foundation for a connected behavioral health system is already here - the focus now is on leveraging it effectively.
Upcoming compliance deadlines highlight the urgency to act. USCDI v3 becomes mandatory on January 1, 2026, and 42 CFR Part 2 single-consent compliance took effect on February 16, 2026 [4]. Relying on outdated, non-interoperable systems increases both regulatory and operational risks.
The way forward is clear: adopt ONC-certified, FHIR-compliant platforms, map out your data workflows, and aim for seamless bidirectional integration across labs, prescribing, referrals, and care coordination. APIs are more than just a technical improvement - they enable behavioral health organizations to provide care that is safer, faster, and more connected.
FAQs
What’s the fastest way to start API interoperability without disrupting care?
Choosing an ONC-certified EHR with support for FHIR-based APIs is the quickest route.
For example, platforms like Opus Behavioral Health EHR align with key standards such as USCDI v3 and 42 CFR Part 2, simplifying processes like e-prescribing, lab integrations, and automated workflows.
This approach removes the need for manual data entry or custom development, ensuring smooth data exchange while preserving continuity of care.
How do APIs handle 42 CFR Part 2 consent for SUD records?
APIs play a key role in meeting the requirements of 42 CFR Part 2 by facilitating consent-driven data segmentation and automating compliance measures. They work by tagging data at the element level, effectively separating general medical information from sensitive Substance Use Disorder (SUD) records.
When a query is made, APIs check the purpose of the request against the patient’s consent to ensure adherence to privacy rules. Additionally, they support security labeling in formats like FHIR, which helps maintain compliance, track disclosures, and ensure the system is auditable.
What KPIs prove an API rollout is actually working?
When introducing an API in behavioral health, it's essential to measure its impact through key performance indicators (KPIs) that reflect both operational and clinical progress.
Some critical metrics to monitor include:
Reduced Administrative Time: Look for decreases in the time spent on tasks like tracking authorizations, which can streamline workflows.
Fewer Medication Errors: Assess whether the API helps minimize errors in prescribing or managing medications.
Improved Real-Time Data Access: Track how efficiently the system retrieves up-to-date information, such as lab results or medication lists.Additionally, keep an eye on declines in manual processes. For instance, fewer phone calls for referrals or less reliance on paper documentation can signal that the API is effectively facilitating smoother care transitions. These metrics provide a clear picture of how well the API supports both staff and patient outcomes.
- Behavioral Health
- EHR Systems
- Addiction Treatment EHR
- Telehealth
- mental health
- addiction treatment
- Behavioral health facility
- behavioral Health center
- HIPPA Compliant
- PTSD
- ehrsoftware
- Depression
- Substance Abuse Disorder
- Anxiety
- MentalHealthMatters
- RCM
- claim denials
- clinical documentation
- hipaa
- mental health awareness
- screening tools

July 28, 2026

July 27, 2026

July 24, 2026

July 23, 2026

July 22, 2026

July 22, 2026
Recommended Posts

Sunday, June 14, 2026
Behavioral Health EHR Certification Explained
Behavioral Health EHR certification ensures that electronic health record systems meet strict standards for privacy, ...

Friday, January 30, 2026
How Customizable EHR Workflows Improve Behavioral Health
Customizable EHR workflows are transforming behavioral health care by simplifying documentation, improving compliance, ...

Wednesday, June 10, 2026
EHR Integration for Pediatric Behavioral Screening Tools
Electronic health record (EHR) systems are transforming pediatric behavioral health care by integrating screening tools ...