
Outdated EHR systems can hurt your practice more than you think.
If your system slows down workflows, struggles with compliance, or lacks modern features like telehealth integration or AI-powered tools, it’s time to reassess.
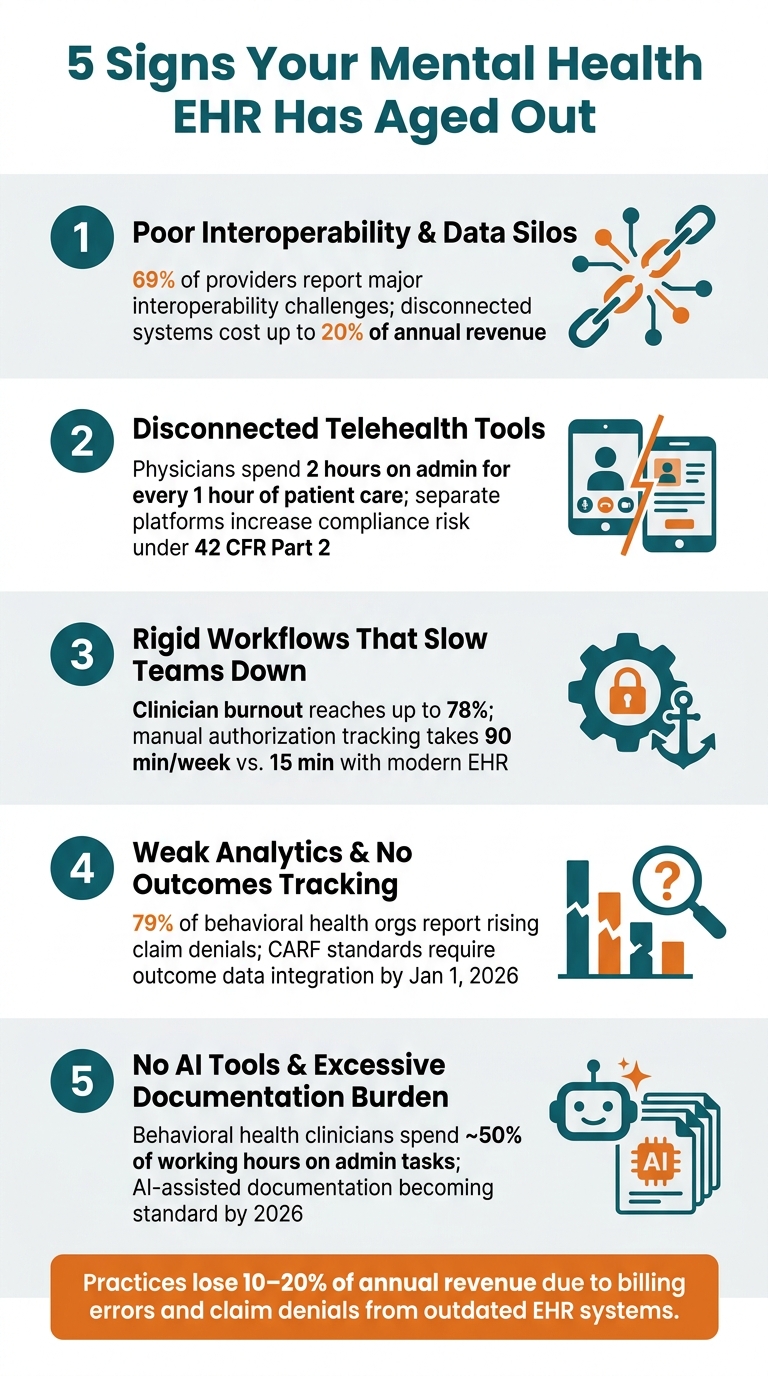
Here are five signs your EHR might be holding you back:
Poor interoperability: Data silos and manual processes lead to inefficiencies, errors, and claim denials.
Disconnected telehealth tools: Juggling multiple platforms wastes time and increases compliance risks.
Rigid workflows: Inflexible systems force workarounds, increasing burnout and documentation delays.
Weak analytics: Limited reporting and outcomes tracking hinder decision-making and compliance.
No AI tools: Excessive manual documentation burdens clinicians and impacts patient care.With new compliance standards like USCDI v3 and 42 CFR Part 2 already in effect for 2026, sticking with an outdated system could lead to financial losses and regulatory issues. A modern EHR can streamline operations, improve patient outcomes, and reduce administrative overhead. Don’t let inefficiencies pile up - evaluate your system today.
5 Signs Your Mental Health EHR Has Aged Out
Sign 1: Poor Interoperability and Data Silos
An outdated EHR system can throw a wrench into everything, from daily administrative work to critical clinical decisions. If your team is still relying on fax machines or manually transferring patient data between systems, it’s a clear sign your EHR is behind the times. 69% of providers report major interoperability challenges with their EHR systems [4]. In behavioral health, these gaps aren’t just inconvenient - they can have serious consequences. This inefficiency wastes time and, more importantly, jeopardizes patient care. Let’s break down how.
How Data Silos Impact Behavioral Health Practices
When clinical notes, billing, scheduling, and intake forms are scattered across disconnected systems, staff often find themselves duplicating tasks. For example, intake staff lose almost two full workdays every week to repetitive data entry and manual insurance verification [5].
The clinical risks are just as concerning. Imagine a prescriber unable to review a therapist's recent session notes or a clinician missing updated medication details during an appointment.
Decisions made with incomplete information can compromise care. And the financial toll? It’s steep. 79% of behavioral health organizations report increasing claim denials due to data gaps, with disconnected systems costing some organizations up to 20% of their annual revenue [5].
"You cannot do this work without data. You cannot fly this plane completely blind." - Dr. Omar Fattal, System Chief of Behavioral Health, NYC Health + Hospitals [5]
What Modern Interoperability Brings to the Table
Modern EHR systems tackle these challenges head-on with seamless integration. They connect labs, pharmacies, and payers using FHIR-based APIs and HL7 standards, enabling real-time data exchange.
This means lab orders and results appear directly in the patient’s chart, e-prescribing includes automated drug interaction alerts, and insurance eligibility checks happen instantly - no more lengthy phone calls.
By January 1, 2026, ONC-certified EHRs must also support USCDI v3, which expands data-sharing to include mental and cognitive health information, addressing behavioral health needs directly [3].
Here’s a quick comparison of outdated systems versus modern solutions:
|
Area |
Outdated EHR |
Modern Standard |
|---|---|---|
|
Medications |
Manual entry, sticky notes |
Integrated e-prescribing with interaction alerts |
|
Labs |
Manual PDF uploads |
In-system lab ordering and results |
|
Payers |
Manual authorization tracking |
Real-time eligibility and automated unit tracking |
|
Intake |
Duplicate data entry across platforms |
Unified patient portal with auto-sync to EHR |
A real-world example highlights the impact: In March 2026, Cleveland Clinic introduced automated prior-authorization systems, speeding up authorization notifications by 6 to 7 days and reducing peer-to-peer review times by 11 days. This improvement directly cut down treatment delays for patients [5]. It’s a clear demonstration of how modern interoperability improves both efficiency and patient care outcomes.
Sign 2: Missing or Disconnected Telehealth Tools
Telehealth has evolved from being a temporary solution to becoming a central part of behavioral health care delivery. If your EHR doesn’t include built-in telehealth functionality, your team is likely juggling multiple platforms to complete a single patient visit - this is a clear sign of an outdated system.
Problems Caused by Separate Telehealth Platforms
When telehealth operates separately from your EHR, it adds layers of complexity to every session. Clinicians are forced to manually transfer notes, log session times, and track billing modifiers. Each manual step increases the risk of errors and compliance issues.
For context, physicians already spend nearly 2 hours on administrative tasks for every 1 hour of direct patient care [1]. A disconnected telehealth system only worsens this imbalance.
The compliance risks are particularly concerning.
For example, under 42 CFR Part 2, substance use disorder (SUD) records require strict confidentiality and explicit patient consent. Standalone telehealth tools often lack the ability to segregate sensitive SUD data, increasing the risk of accidental disclosure.
Similarly, the 21st Century Cures Act mandates that patients have seamless access to their electronic health information. Fragmented systems can inadvertently block this access, potentially leading to regulatory penalties.
"Fragmented documentation makes audits harder and creates gaps in the evidence packages that CARF and Joint Commission reviewers expect to see." - Cara Cragun, Author, Alleva [6]
These challenges don’t just complicate compliance - they also disrupt daily workflows. For example, when appointment reminders and session links need to be sent manually or through a separate system, patients are more likely to miss their sessions.
Integrated systems, on the other hand, automate these reminders with secure session links, which can significantly reduce no-show rates [2][4].
Why Telehealth Should Be Built Into Your EHR
An EHR with native telehealth functionality eliminates the inefficiencies caused by bolt-on tools. With everything - video sessions, scheduling, documentation, and billing - housed in one system, clinicians can access a patient’s full chart during a call, sync consent forms automatically, and ensure claims are processed with the correct modifiers.
This streamlined approach removes the daily frustrations caused by disconnected systems and supports the efficiency modern behavioral health care requires.
"If you're switching between platforms mid-session or troubleshooting video connections every week, your EHR wasn't designed for telehealth; it was adapted for it." - The PIMSY Team [2]
The table below highlights key differences between standalone telehealth platforms and EHRs with native telehealth, showing how these gaps affect day-to-day operations:
|
Feature |
Standalone Telehealth Platform |
Native EHR Telehealth |
|---|---|---|
|
Data Entry |
Manual transfer of notes and session times |
Automatic syncing to patient record |
|
Scheduling |
Double-entry across two systems |
Single-entry; auto-updates calendar |
|
Patient Experience |
Multiple logins and portals |
Single portal for forms, links, and billing |
|
Billing |
Manual tracking of modifiers |
Automated claim scrubbing and modifiers |
|
Clinical Context |
Limited access to history during call |
Real-time access to full chart and labs |
If your team has to switch between platforms just to complete a telehealth session, this structural flaw is likely creating daily operational headaches.
Sign 3: Rigid Workflows That Slow Your Team Down
An outdated EHR can feel like an anchor, dragging down both efficiency and patient care. While disconnected telehealth tools might disrupt individual sessions, rigid workflows create ripple effects that impact every aspect of operations - scheduling, documentation, billing, and supervision. Over time, these inefficiencies pile up, creating significant bottlenecks.
How Rigid Workflows Affect Clinical and Administrative Teams
Many older EHR systems were designed with primary care in mind, focusing on quick 15-minute visits and brief, standardized notes. But behavioral health operates differently. A typical 50-minute therapy session requires rich, narrative documentation.
When clinicians are forced into templates that don’t align with their needs, they often turn to workarounds like spreadsheets, sticky notes, or manual exports. These "shadow systems" are a clear sign the EHR isn’t meeting the demands of the practice.
This mismatch is especially problematic in behavioral health, where documentation requirements are more intensive, and burnout is alarmingly high - reaching up to 78% among clinicians [7].
An EHR that adds complexity instead of reducing it only worsens the strain. Rigid workflows designed for other specialties make it harder for clinicians to meet behavioral health’s unique documentation standards, creating unnecessary friction.
"The true cost of time dedicated to EHR documentation work is even greater than previously thought. Documentation burden is a real barrier to other EHR-based tasks that improve care and reduce costs." - Jay Holmgren, PhD, MHI, Director of the UCSF Center for Clinical Informatics and Improvement Research [5]
Supervision is another area where outdated systems fall short. Without a streamlined review-and-sign process, supervisors waste time chasing down notes, delaying compliance reporting and slowing down care.
On top of that, manual billing calculations - based on service types and hours worked - consume valuable time and increase the chance of errors. These inefficiencies highlight the need for more flexible, automated workflows.
What Configurable and Automated Workflows Can Do
Modern EHRs provide the flexibility and automation needed to eliminate these bottlenecks. Instead of locking clinicians into rigid, one-size-fits-all processes, they offer configurable tools like customizable forms, task triggers, and role-based dashboards.
And the best part?
These updates don’t require custom coding or months of development [8].
For example, once a note is completed, the system can automatically route it for review or generate tasks when authorizations are nearing their limits - no more relying on spreadsheets.
The impact of these improvements is tangible. In February 2026, a behavioral health practice in Greenville with 20 clinicians transitioned away from manual authorization tracking.
As a result, they cut task time from 90 minutes to just 15 minutes per week [3]. This kind of efficiency doesn’t just save time - it allows clinicians to focus more on patient care. By reducing unnecessary clicks and cognitive overload, modern EHRs help restore productivity and enhance the quality of care clinicians can provide.
Sign 4: Weak Analytics and No Outcomes Tracking
When leadership decisions are based on incomplete data, it's often because the EHR system lacks the ability to provide automated insights. Without this capability, decisions are made without a full understanding of the situation.
The Impact of Poor Analytics on Behavioral Health Organizations
A lack of clear, actionable data creates serious challenges. Without integrated reporting tools, practice leaders struggle to evaluate which programs are thriving, whether clinicians are meeting documentation goals, or where financial losses are occurring. Alarmingly, 79% of behavioral health organizations have reported an increase in claim denials due to gaps caused by disconnected systems [5].
Tracking patient outcomes is another area that suffers. Older systems often require clinicians to manually enter standardized assessments - like PHQ-9 or GAD-7 - into separate spreadsheets. This makes it incredibly difficult to monitor a patient’s progress over time [2][9].
Beyond inefficiency, this creates compliance risks. Starting January 1, 2026, CARF accreditation standards will require organizations to show that outcome data is directly influencing treatment decisions [5]. If your EHR system can't generate outcome reports automatically, your compliance efforts could fall short. Advanced analytics can close this gap, making decision-making more efficient and effective.
Key Features of Strong Analytics and Reporting
Modern EHR systems are designed to address these issues with features like:
Self-service reporting tools that include customizable templates
Real-time dashboards showing metrics such as clean claim rates and clinician productivity
The ability to break down data by provider, location, or service line [4][10]On the clinical side, having built-in assessments with automatic scoring and trend visualization is critical. Clinicians should be able to view a patient’s PHQ-9 progress directly within their chart, without needing to search through separate files.
For financial management, advanced systems can track key metrics such as days in accounts receivable (A/R), first-pass resolution rates, and payer-specific reimbursement trends - all without requiring custom reporting [10].
Additionally, outcome reports should align seamlessly with CARF and other accreditation standards, embedding compliance into daily operations. If your current system requires cumbersome workarounds to achieve these capabilities, it might be time to consider an upgrade.
Sign 5: No AI Tools and Too Much Documentation Work
If your EHR system makes documentation more complicated instead of simplifying it, it’s a clear sign your system is outdated. Behavioral health clinicians spend nearly 50% of their working hours on administrative tasks - about twice as much as primary care physicians [9]. Without tools to ease this burden, productivity takes a hit.
The Cost of Manual Documentation and Clunky Interfaces
Older EHR systems often rely on outdated methods like free-text fields, rigid templates, and interfaces that require excessive clicks to complete even simple tasks.
These inefficiencies don’t just slow down workflows; they push staff to create workarounds like spreadsheets, sticky notes, or manual data entry. While these makeshift solutions might seem helpful in the moment, they waste time, increase the risk of documentation errors, and scatter important data across multiple platforms.
The result? Clinicians spend more time battling with software than caring for patients. Over time, this frustration can lead to burnout and even staff turnover - problems that behavioral health organizations can’t afford to ignore.
How AI-Powered Documentation Makes a Difference
Modern AI tools are changing the game, making documentation more efficient and less stressful. The latest EHR systems incorporate AI-assisted features that help clinicians complete notes faster while keeping control of the clinical narrative.
These tools don’t replace the clinician’s expertise - they support it.
Take Opus’s Copilot AI as an example. It’s built to help clinicians streamline documentation without sacrificing clinical judgment. By 2026, AI-assisted documentation is expected to become a standard feature, essential for reducing the manual workload [9].
If your EHR doesn’t offer this capability, it’s likely falling behind. A great way to test this during a demo is to have a clinician complete a real DAP or SOAP note using the AI tools and see how much time and effort is saved [9].
Improving documentation is just the start - next, it’s worth examining your entire EHR workflow to identify where upgrades are most needed.
How to Assess Your Current EHR and Plan Next Steps
Spot daily inefficiencies and create a focused plan for improvement.
Running an EHR Workflow Audit
An EHR workflow audit doesn’t have to be complicated. The main idea is simple: document every workaround happening in your practice. Start by observing a typical day with your front-desk staff, billers, and clinicians individually.
Each group might face unique challenges that leadership may not be aware of.
For example, reliance on shadow systems is a clear sign of EHR inefficiency. If a clinician copies session notes into a Word document before pasting them back into the system, that’s a shadow system. Similarly, exporting data to Excel manually is another workaround.
These workarounds highlight gaps where your current EHR is falling short.
Also, take note of after-hours documentation. In behavioral health, clinicians often spend 1 to 2 hours on documentation for every hour of direct patient care [5]. Tracking this time provides a solid metric to present to leadership when advocating for change.
Here’s a quick comparison of outdated systems versus modern solutions across key audit categories:
|
Audit Category |
Red Flag (Outdated) |
Modern Standard |
|---|---|---|
|
Telehealth |
Separate platform; manual syncing |
Built-in integration; one-click sessions |
|
Documentation |
Rigid templates; excessive clicks |
AI-assisted scribes; flexible narrative tools |
|
Reporting |
Manual Excel exports |
Real-time, customizable dashboards |
|
Interoperability |
Faxes and phone calls for records |
HL7/FHIR standards for secure data sharing |
|
Billing |
Manual code updates; high denials |
Automated billing with built-in rules |
These findings will help guide the next step: defining your EHR requirements.
Building an EHR Requirements Checklist
Once you’ve identified the pain points, turn them into must-have features for your next EHR. Each issue uncovered during the audit should directly translate into a requirement.
For instance, if your team manually verifies insurance eligibility, you’ll want "automated eligibility verification" on your checklist. If clinicians rely on a separate telehealth platform, native telehealth integration becomes non-negotiable.
A smart way to organize this is by creating a weighted scorecard with 8–10 critical criteria, such as compliance with 42 CFR Part 2 for substance use records, integrated billing, AI-powered documentation, and tools for tracking outcomes like PHQ-9 and GAD-7 dashboards [11].
Scoring vendors immediately after demos ensures evaluations remain fair and that flashy features don’t overshadow essential needs.
"The true cost of time dedicated to EHR documentation work is even greater than previously thought. Documentation burden is a real barrier to other EHR-based tasks that improve care and reduce costs." - Jay Holmgren, PhD, Director of the UCSF Center for Clinical Informatics and Improvement Research [5]
With a detailed checklist, you’ll have the evidence you need to justify investing in a better system.
Making the Case for Upgrading to a Modern Behavioral Health EHR
The best case for upgrading isn’t just about better technology - it’s about the impact on finances, staff retention, and patient care. For example, behavioral health practices lose 10% to 20% of their annual revenue due to billing errors and claim denials [5].
On top of that, replacing a clinician who leaves due to burnout costs between $30,000 and $50,000 [5]. These are real, ongoing losses that add up every year you stick with an outdated system.
Now, compare those losses to the one-time costs of upgrading. For a small practice, migrating to a modern platform - including data transfer and retraining - typically costs $5,000 to $25,000 [12].
When you weigh these numbers, it’s hard to justify sticking with an inefficient system. Solutions like Opus Behavioral Health EHR are specifically designed for behavioral health teams, offering features like group therapy documentation, DSM-5 templates, residential bed management, and Copilot AI - all tailored to fit your workflows [2][5].
Conclusion: Spotting an Outdated EHR and Doing Something About It
Outdated EHR systems come with telltale signs: isolated data silos, clunky telehealth integration, rigid templates, lack of real-time outcomes tracking, and documentation processes that stretch clinicians' work hours - all of which inflate costs. Behavioral health organizations sticking with these aging systems risk losing 3% to 5% of annual revenue due to manual workarounds alone [5].
Starting January 1, 2026, CARF standards will mandate outcome data integration. If your EHR can't show real-time trends for tools like PHQ-9 or GAD-7, your practice could face compliance issues. Recognizing these risks is the first step toward taking action.
A workflow audit can help identify where your system falls short, while a weighted checklist of requirements can guide your evaluation process.
When you compare the costs of turnover and compliance risks to the one-time expense of upgrading, the numbers often speak for themselves. For example, Opus Behavioral Health EHR is designed specifically for behavioral health teams, offering tools like Copilot AI, DSM-5 templates, and integrated outcomes tracking.
These features address common pain points such as data silos, telehealth inefficiencies, rigid workflows, and the documentation burden.
The longer you hold on to an outdated system, the more it costs - not just financially, but also in staff morale and patient care quality. The first step? Take a close look at your current EHR's strengths and weaknesses and decide if it's time for a change.
FAQs
How can I tell if my EHR’s interoperability is affecting revenue?
Poor system integration can create fragmented workflows and cost your practice money. Common warning signs include repeated manual data entry, billing mistakes, claim denials, and wasted administrative hours.
When clinical documentation and billing systems don’t communicate effectively, delays pile up, and compliance risks grow.
If your team has to switch between multiple systems just to complete routine tasks, the inefficiencies and extra workload can take a toll. In fact, many practices lose 10%-20% of their annual revenue due to these issues.
What telehealth features should be native in a behavioral health EHR?
A modern behavioral health EHR needs built-in telehealth capabilities to simplify workflows and improve efficiency. Key features to prioritize include:
In-system scheduling: This allows you to manage appointments directly within the EHR, saving time and reducing the chances of errors.
One-click virtual session access: Streamlined access ensures both providers and clients can join sessions without technical hiccups.
Automated documentation syncing: Automatically linking session notes and records to the patient’s file reduces manual work and keeps everything organized.Additionally, having secure messaging tools for team communication enhances collaboration, while FHIR-based APIs ensure seamless, real-time data exchange with other systems, patient portals, and health networks. Native integration is crucial for reducing administrative tasks and avoiding potential data loss, making your workflow smoother and more reliable.
How can I run a quick workflow audit before deciding to upgrade?
Mapping out your current workflows is a great starting point. Begin by gathering feedback from your staff about the challenges they face daily. Look for recurring pain points, workarounds they’ve developed, tasks that eat up too much time, and how many systems they have to juggle each day.
Pay close attention to key metrics like how long it takes to document each patient visit and how many appointments your team can handle in a day.
Using this information, put together a checklist that clearly shows where your current system is falling short and where it’s actually helping your operations run smoothly. This will give you a clear picture of what needs improvement.
- Behavioral Health
- EHR Systems
- Addiction Treatment EHR
- Telehealth
- mental health
- addiction treatment
- Behavioral health facility
- behavioral Health center
- ehrsoftware
- HIPPA Compliant
- PTSD
- Substance Abuse Disorder
- Depression
- hipaa
- Anxiety
- MentalHealthMatters
- RCM
- claim denials
- clinical documentation
- mental health awareness
- screening tools

August 06, 2026

August 05, 2026

August 04, 2026

August 03, 2026
July 31, 2026

July 30, 2026
Recommended Posts

Wednesday, June 17, 2026
The Hidden ROI of Getting Your Mental Health EHR Right
When it comes to mental health EHR systems, the true value lies in more than just reducing documentation time or ...

Tuesday, June 09, 2026
EHR Mental Health Platforms That Reduce Admin Burden
Behavioral health providers spend 37% of their time on administrative tasks like documentation, cutting into patient ...

Monday, June 15, 2026
Essential Features in Mental Health EHR Systems
Mental health EHRs are specialized tools designed for behavioral health professionals, addressing unique challenges ...